
Thorax — MCQs

On this page
Which particle size is most dangerous in causing pneumoconiosis?
The supraventricular crest is located between which of the following structures?
A 30-year-old man came with choking episodes after ingestion of fish bone while eating. The fishbone got impacted at the level of T4 in the esophagus. Which is the most likely site of obstruction?
While doing an endoscopy, constriction is felt at the oesophageal junction at 25 cm from the incisor. This is due to?
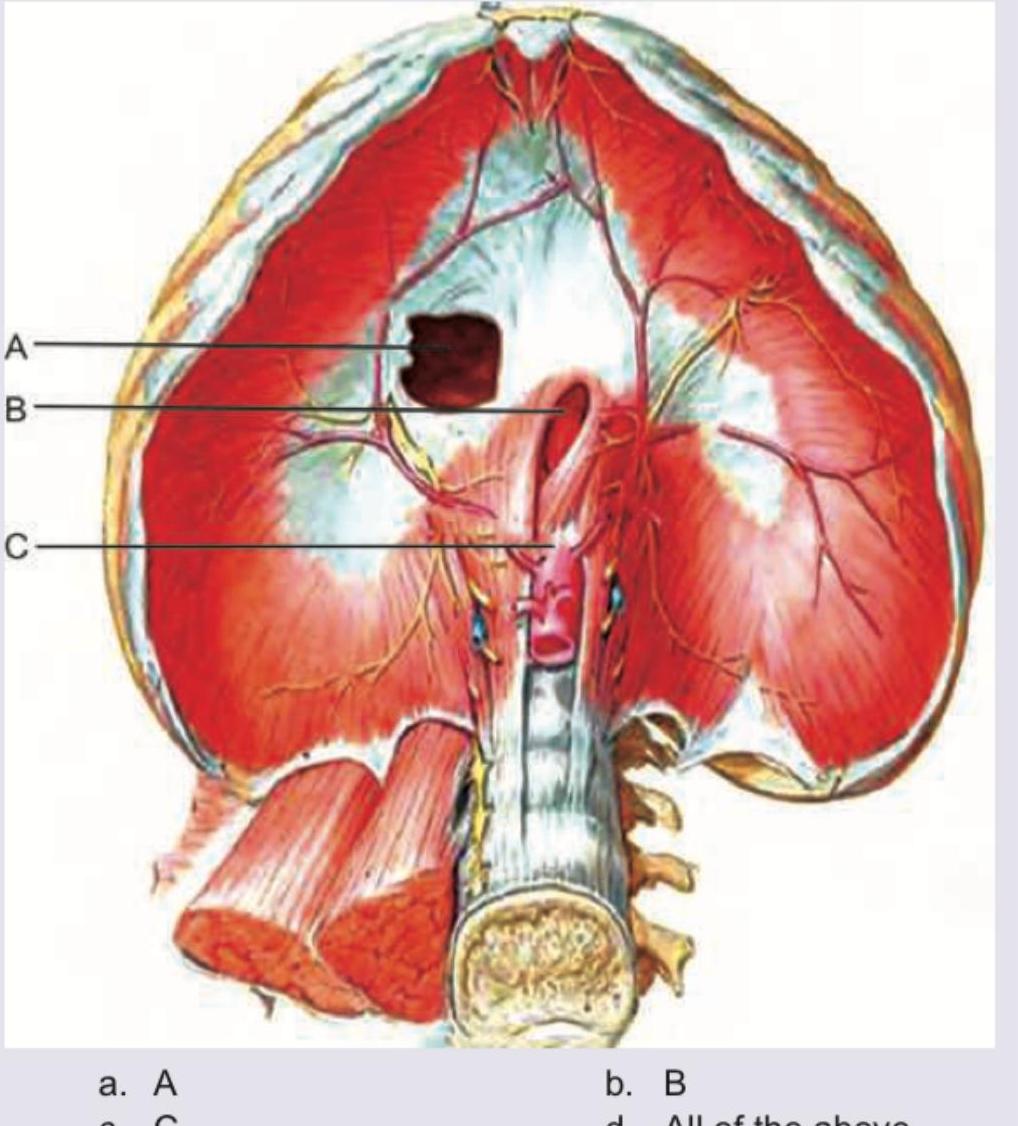
Which of the following structures passes through the foramen marked by the arrow? 
Match the cardiac anatomical features from Column I with their corresponding labels from Column II. Column I: 1. Receives oxygenated blood from pulmonary veins; 2. Lies anterior to ascending aorta; 3. Arises from LV; 4. Hypertrophy in pulmonary stenosis. Column II: A. Ascending aorta; B. Right ventricle; C. Pulmonary trunk; D. Left atrium.
The contraction of the diaphragm has no effect on which of the following apertures in the diaphragm?
The commonly seen depression deformity of the chest wall is known as
Inhaled foreign bodies are more likely to get lodged in the right main bronchus because
Consider the following statements: Venacaval opening of the diaphragm, situated at the level of T8 transmits 1. inferior vena cava 2. vagus nerve 3. branches of the right phrenic nerve 4. thoracic duct Which of the statements given above are correct?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app