
Thorax — MCQs

On this page
Which of the following vessels is typically injured in a patient with hemothorax?
The bronchial artery supplies all of the following except:
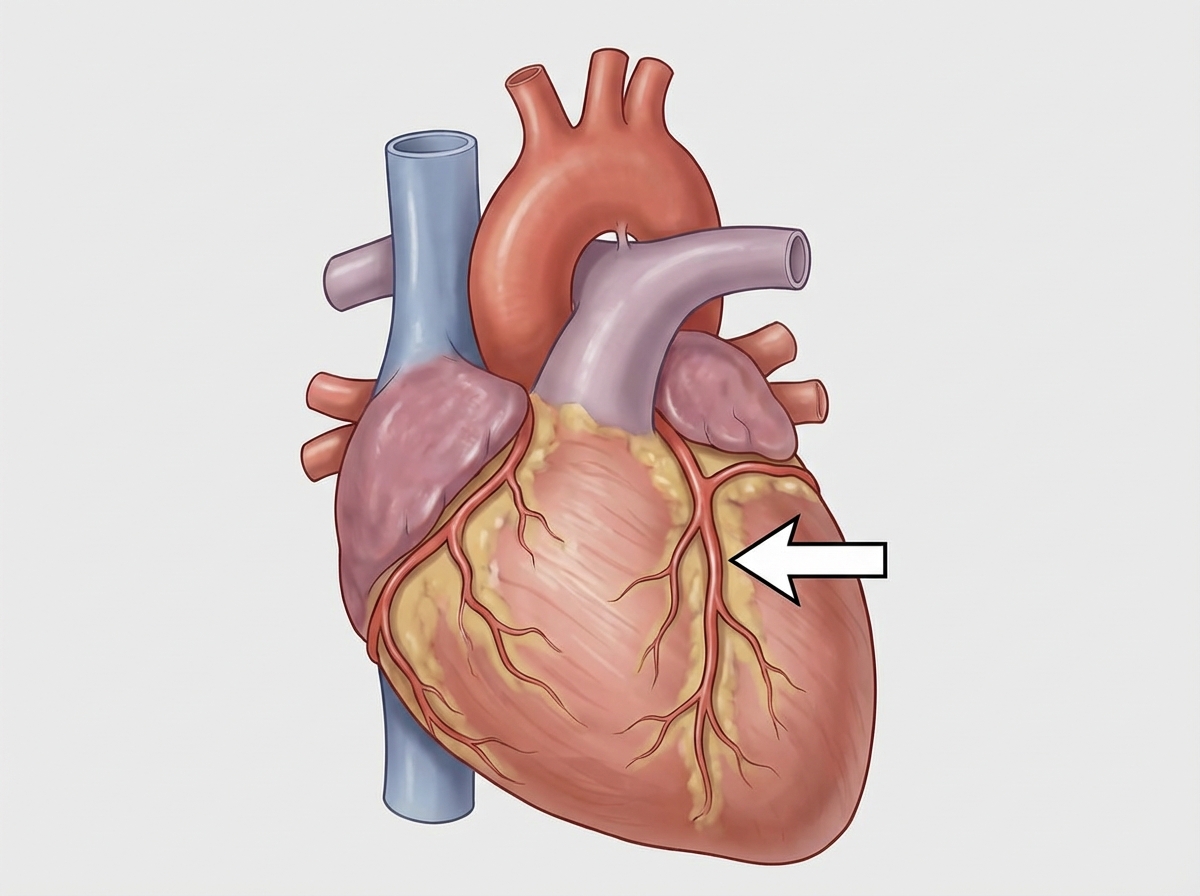
The structure marked with an arrow is:
Torus aorticus involves which structure?
Which of the following does NOT supply the oesophagus?
What is the root value of the intercostobrachial nerve?
Which muscle causes opening of the upper end of the esophagus?
Which nerve supplies the serratus anterior muscle?
A 35-year-old woman is admitted to the hospital with a complaint of shortness of breath. During physical examination, it is noted that there is wide splitting in her S2 heart sound. Which of the following valves is/are responsible for the production of the S2 heart sound?
Several weeks after surgical dissection of her left axilla for the removal of lymph nodes for staging and treatment of her breast cancer, a 32-year-old woman presented with "winging" of her left scapula when pushed against resistance. She also reported difficulty raising her right arm above her head. A nerve was accidentally injured during the surgical procedure, causing the scapular abnormality and inability to raise her arm normally. What was the origin of this injured nerve?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app