
Thorax — MCQs

On this page
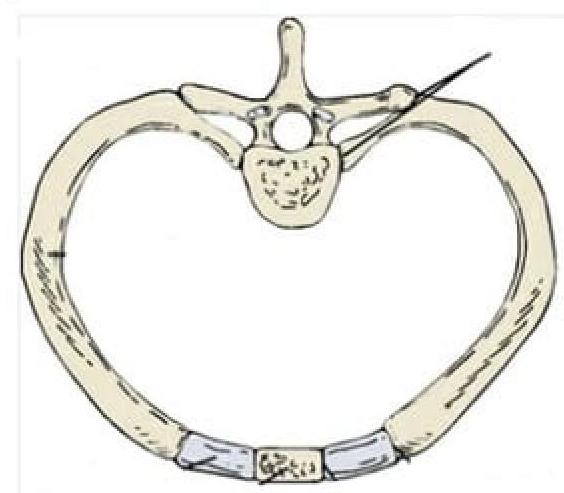
Identify the type of joint in the image provided.
Which of the following statements about Sibson's fascia is correct?
What type of joint is formed by the costal cartilages of the 8th and 9th ribs?
Which of the following structures does not pass through the aortic opening?
Which of the following is not seen in the anterior mediastinum?
Anterior Mediastinal nodes are included in which level of lymph nodes?
Food can commonly get obstructed in the esophagus at all of the following locations except
Which is the narrowest portion of the esophagus?
Arch of aorta begins at which vertebral level?
Which artery supplies the anterior part of the interventricular septum?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app