
Thorax — MCQs

On this page
Which of the following structures is not related to the first rib?
Which anatomical structure is located posterior to the transverse pericardial sinus?
What is the typical number of lactiferous ducts that open in the nipple?
Posterior relation of hilum of the lung?
Which of the following structures is not associated with the hilum of the right lung?
What is the anatomical origin of the thoracic duct?
Thoracic duct opens into ?
Xiphoid fuses with sternum by what age?
Which of the following statements is true regarding the right principal bronchus?
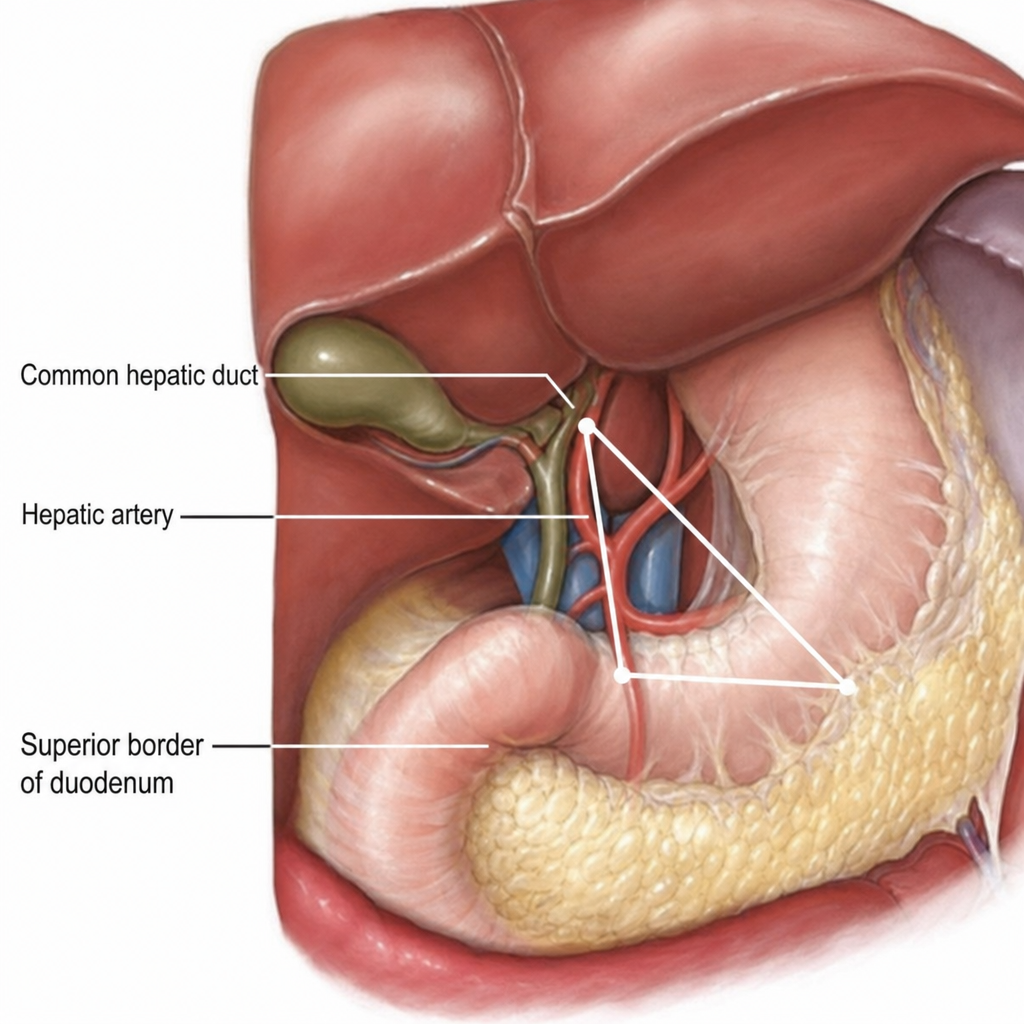
Identify the triangle in the image below.
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app