
Thorax — MCQs

On this page
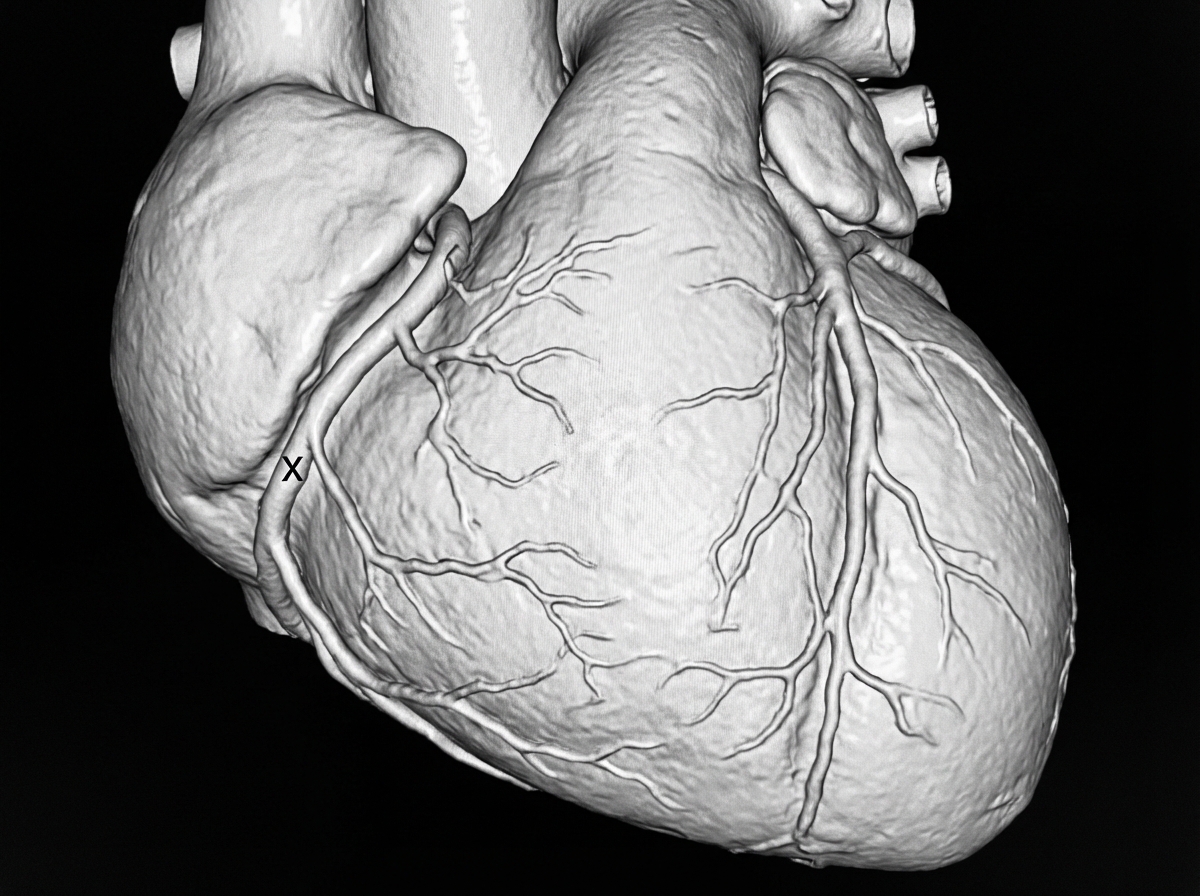
A Coronary CT angiogram shows a blood vessel marked as 'X' coursing around the right side of the heart. Small branches originating from this vessel supply the lateral surface of the heart and are called acute marginal branches. Identify the vessel marked as 'X'.
The commonly seen depression deformity of the chest wall is known as
Inhaled foreign bodies are more likely to get lodged in the right main bronchus because
Dysphagia lusoria is a condition which results from
Consider the following statements: Venacaval opening of the diaphragm, situated at the level of T8 transmits 1. inferior vena cava 2. vagus nerve 3. branches of the right phrenic nerve 4. thoracic duct Which of the statements given above are correct?
Arrange lung hilar structure from anterior to posterior:- 1. Primary bronchus 2. Bronchial artery 3. Pulmonary vein 4. Pulmonary artery
During a thoracotomy procedure, a surgeon needs to access the posterior mediastinum. Which of the following structures forms the anterior boundary of the posterior mediastinum?
A 56-year-old man is brought to the emergency department 30 minutes after falling from a height of 3 feet onto a sharp metal fence pole. He is unconscious. Physical examination shows a wound on the upper margin of the right clavicle in the parasternal line that is 3-cm-deep. Which of the following is the most likely result of this patient's injury?
NOT a content of superior mediastinum
Left anterior descending artery is a direct branch of
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app