
Thorax — MCQs

On this page
Which of the following is NOT a tributary of the Azygos Vein?
The right coronary artery arises from which aortic sinus?
Which of the following vessels is typically injured in a patient with hemothorax?
The bronchial artery supplies all of the following except:
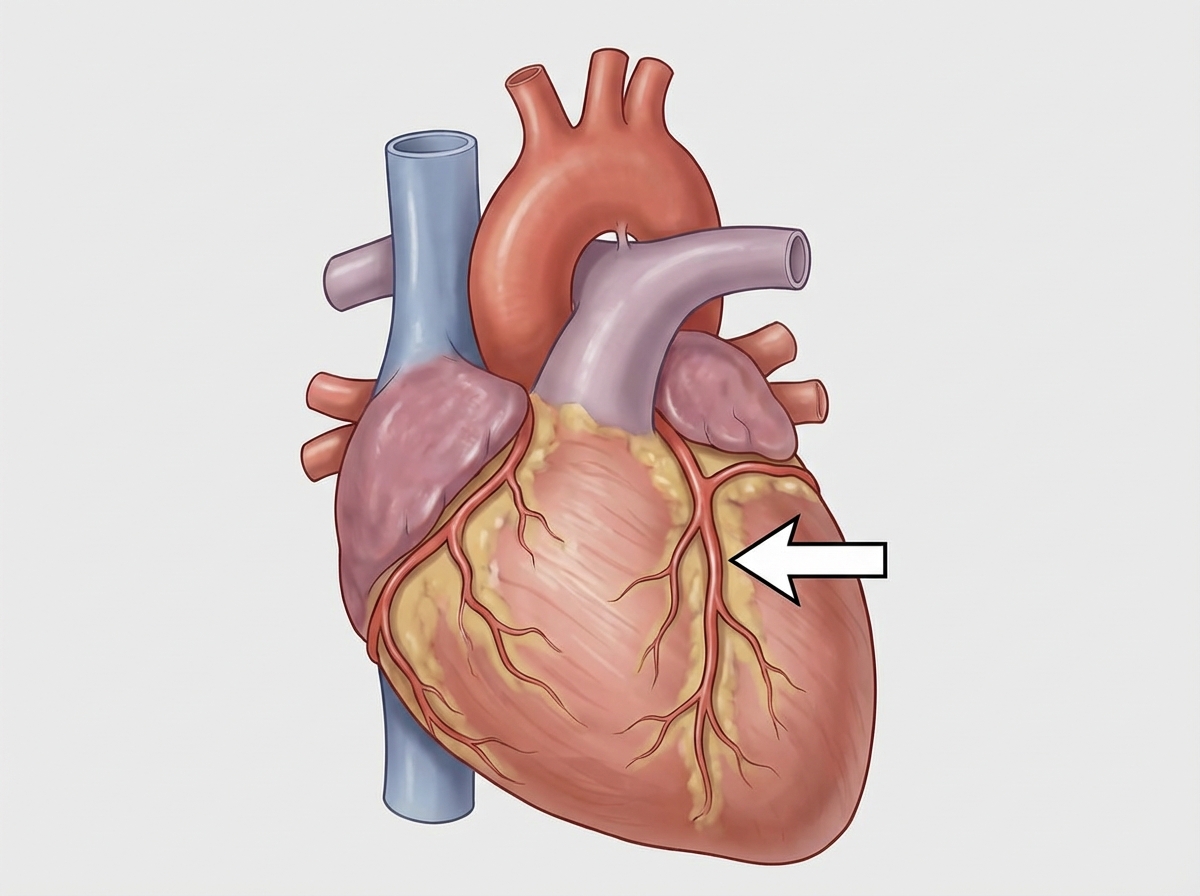
The structure marked with an arrow is:
A patient presents with carcinoma in the upper outer quadrant of the breast. Which of the following lymph node groups is LEAST likely to be a site of metastasis?
Which of the following does NOT supply the oesophagus?
The coronary sinus:
The hemiazygos vein crosses from left to right at which vertebral level?
What is the lymphatic drainage of the upper outer quadrant of the breast?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app