
Thorax — MCQs

On this page
All of the following are branches of the internal thoracic artery except?
A patient presents with a penetrating chest wound associated with intrathoracic hemorrhage. A thoracotomy is performed via an incision in the 4th/5th intercostal space, starting 1 cm away from the lateral margin of the sternum. This approach is taken to avoid injury to which of the following structures?
Which among the following is a typical intercostal nerve?
A 37-year-old woman undergoes a routine breast examination. The physician notes that the skin of the breast moves with the underlying breast tissue, indicating normal attachment. What anatomical structures are responsible for this normal attachment of the breast tissue to the overlying skin?
What is the primary blood supply to the thoracic part of the esophagus?
The great cardiac vein drains into which structure?
What is a typical feature of thoracic vertebrae?
The base of the heart is typically located at the level of which vertebrae?
What anatomical structure is located posterior to the sternum?
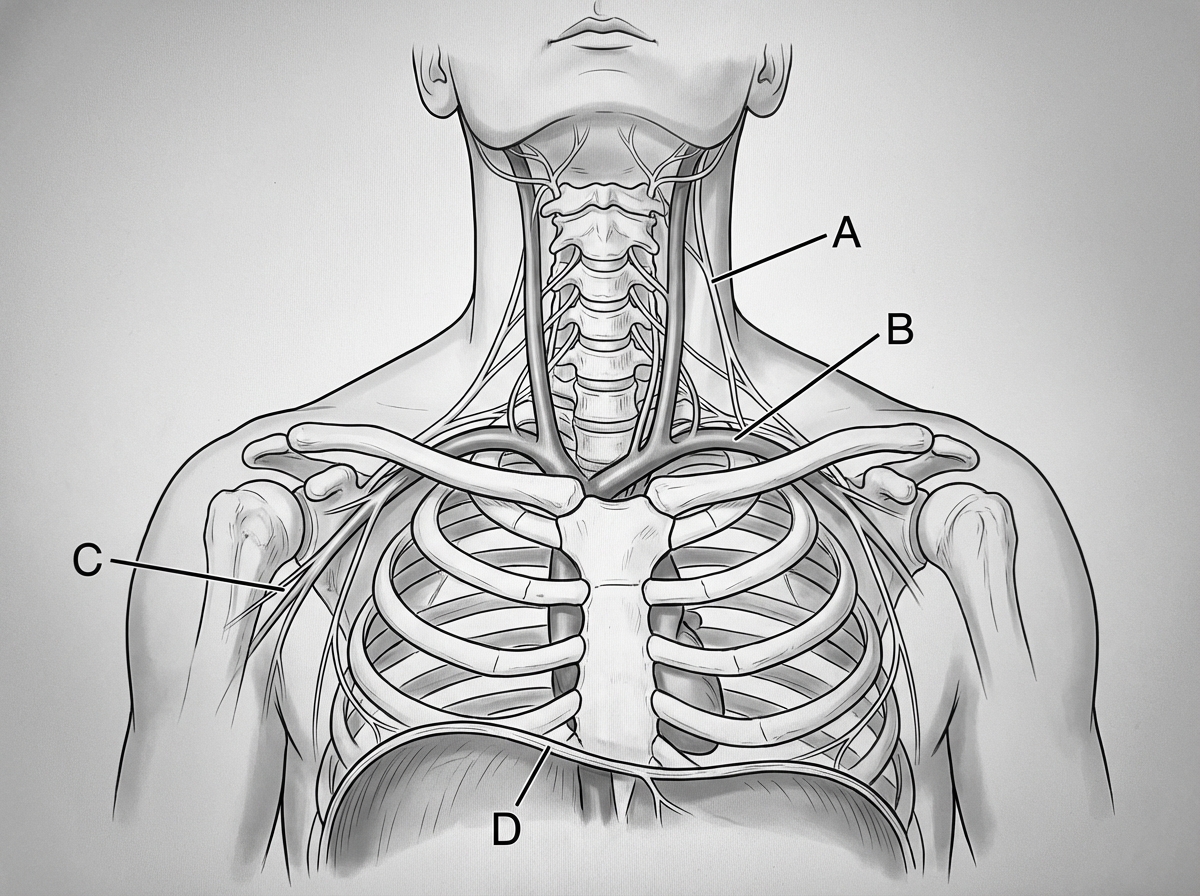
Injury to which of the following nerves, as indicated in the diagram, may cause diaphragmatic paralysis?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app