
Thorax — MCQs

On this page
A 35-year-old female is admitted to the emergency department because of cardiac arrhythmia. ECG examination reveals that the patient suffers from atrial fibrillation. Where is the mass of specialized conducting tissue that initiates the cardiac cycle located?
Which of the following structures does not pass through the thoracic inlet?
The first rib articulates with the sternum in close proximity to which structure?
In evaluating a breast lesion located in the anterior axillary line, to which site does the lateral edge of normal breast tissue extend?
The thoracic duct does not drain which of the following regions?
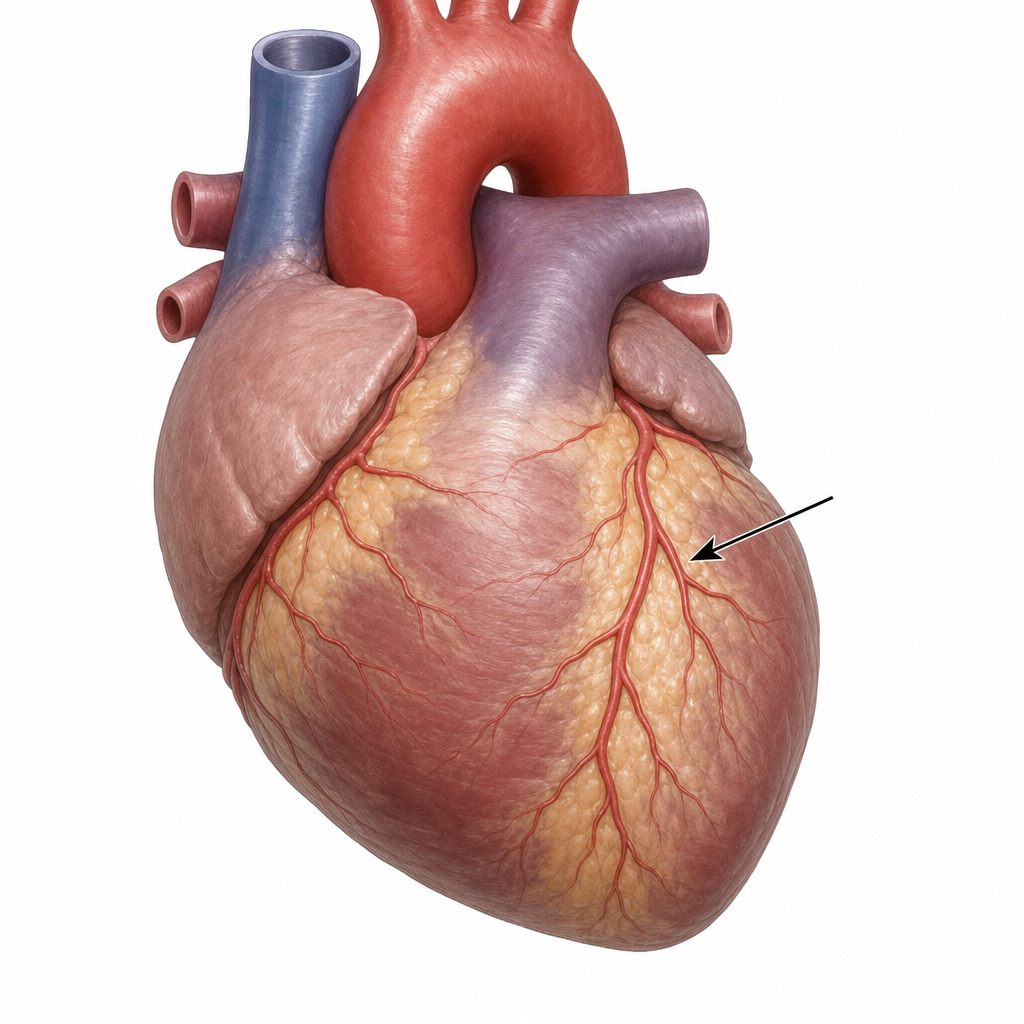
The vessel shown in the diagram is a branch of:
Blood supply of the diaphragm is through all of the following, except?
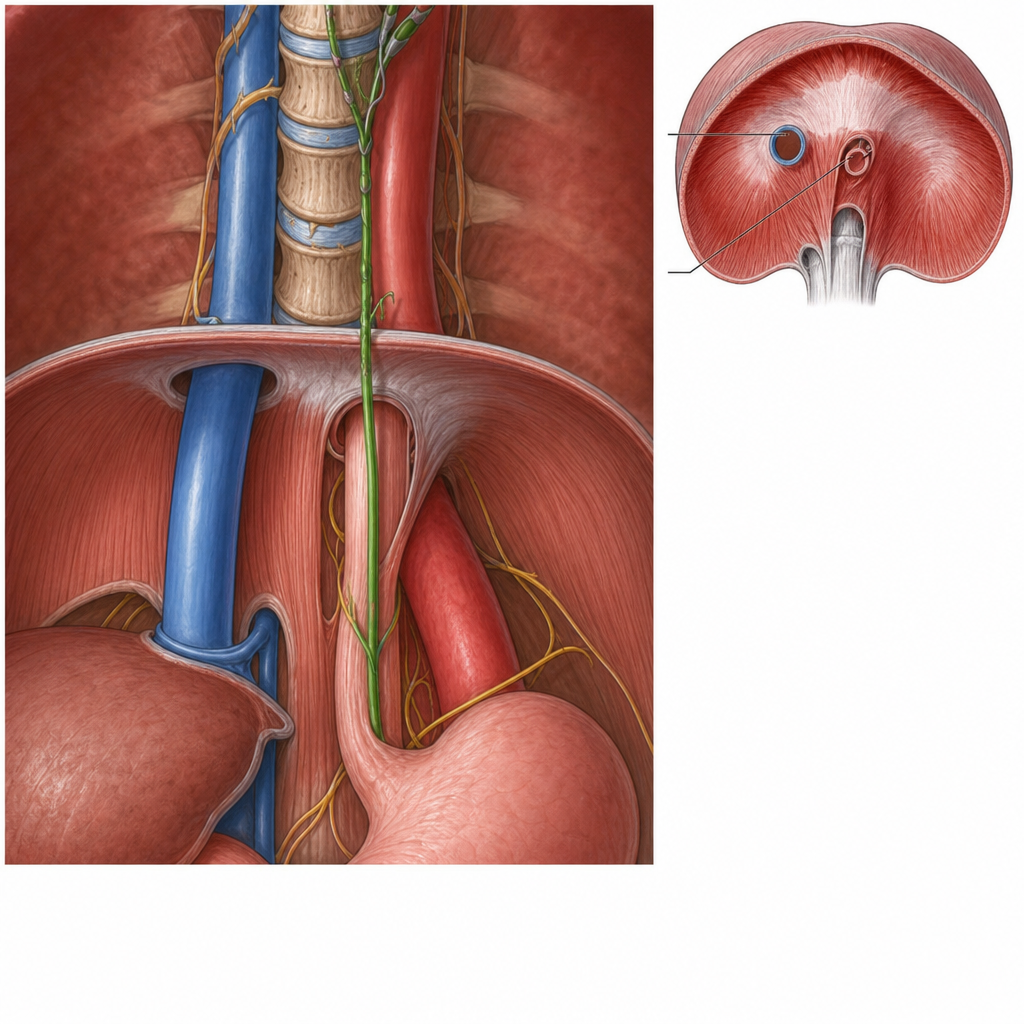
The aortic opening of the diaphragm transmits which of the following structures?
What is the distance of the lower esophageal sphincter from the upper incisors?
Which of the following statements regarding the SA node is incorrect?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app