
Thorax — MCQs

On this page
Which structure passes through the central tendon of the diaphragm?
Which channel drains the major part of the myocardium?
Needle for thoracocentesis is inserted most commonly at which anatomical location?
A 32-year-old male janitor complains of a swollen face during the past week. A CT scan reveals an expanding hematoma in the superior mediastinum. Mediastinal tamponade is most likely to manifest as which of the following?
Which of the following statements regarding the diaphragm are true? (a) The right crus is shorter than the left crus. (b) The esophagus passes through the diaphragm at the level of T10. (c) The inferior vena cava passes through the diaphragm at the level of T10. (d) The aorta passes through the diaphragm at the level of T8. (e) The diaphragm is the primary muscle of inspiration.
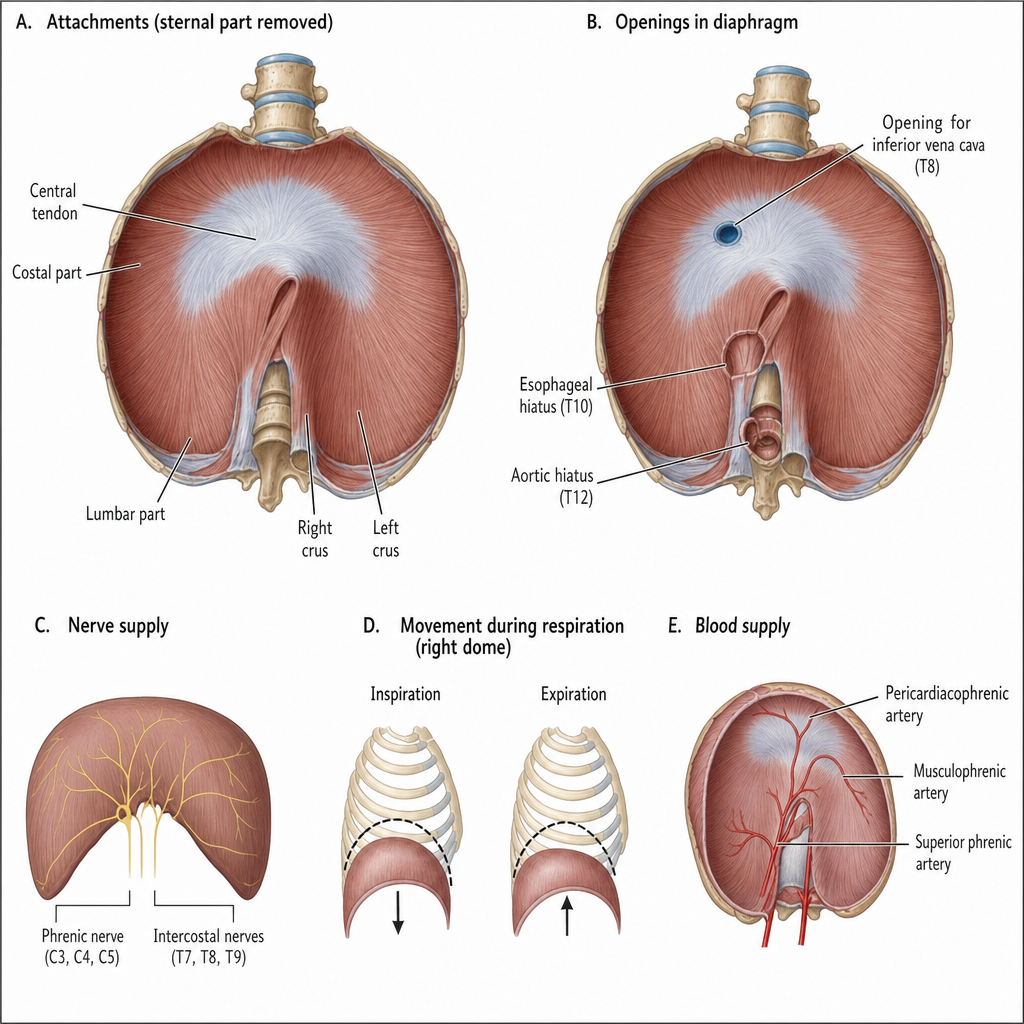
At which vertebral level does the inferior vena cava pass through the diaphragm?
Which of the following muscles attaches to the first rib?
What is the name of the pleura that covers the surface of the lungs?
Diaphragmatic hernias can occur through all of the following anatomical structures EXCEPT:
Which tissue undergoes cyclic changes in women's breasts?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app