
Thorax — MCQs

On this page
The nipple is supplied by which of the following intercostal nerves?
In which intercostal space is the typical arrangement of vein, artery, and nerve (VAN) absent?
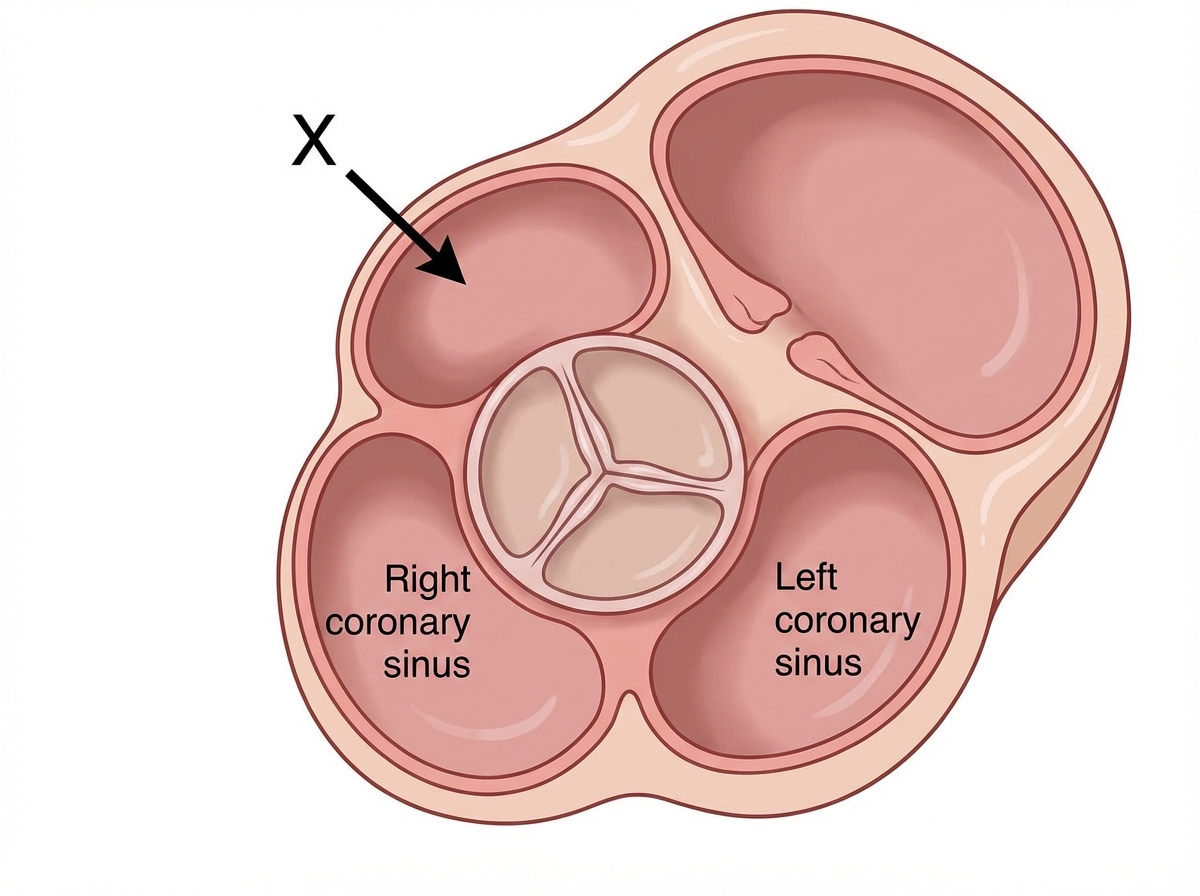
Which of the following structures form the bulge marked X?
Which of the following is NOT pierced during pleural tapping?
Which of the following statements is NOT true?
Which chamber forms the base of the heart?
A child is eating while lying supine in bed and aspirates a peanut. Which bronchopulmonary segment is this foreign object most likely to enter?
The subcostal nerve lies at:
A 46-year-old patient presents with complaints of chest pain and headache. A computed tomography (CT) scan reveals a tumor located just superior to the root of the right lung. Blood flow in which of the following veins is most likely blocked by this tumor?
During a mastectomy on a 60-year-old female patient, which artery gives origin to the small branches supplying the medial side of the breast?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app