
Thorax — MCQs

On this page
Which of the following is NOT found in the posterior mediastinum?
Which artery is most commonly occluded in an inferior wall myocardial infarction?
All of the following are true about the thymus, EXCEPT:
Which of the following structures does NOT cause constriction of the esophagus?
In a patient with a tumor in the superior mediastinum compressing the superior vena cava, all of the following veins would serve as alternate pathways for blood return to the right atrium, except?
The breast is classified as which of the following?
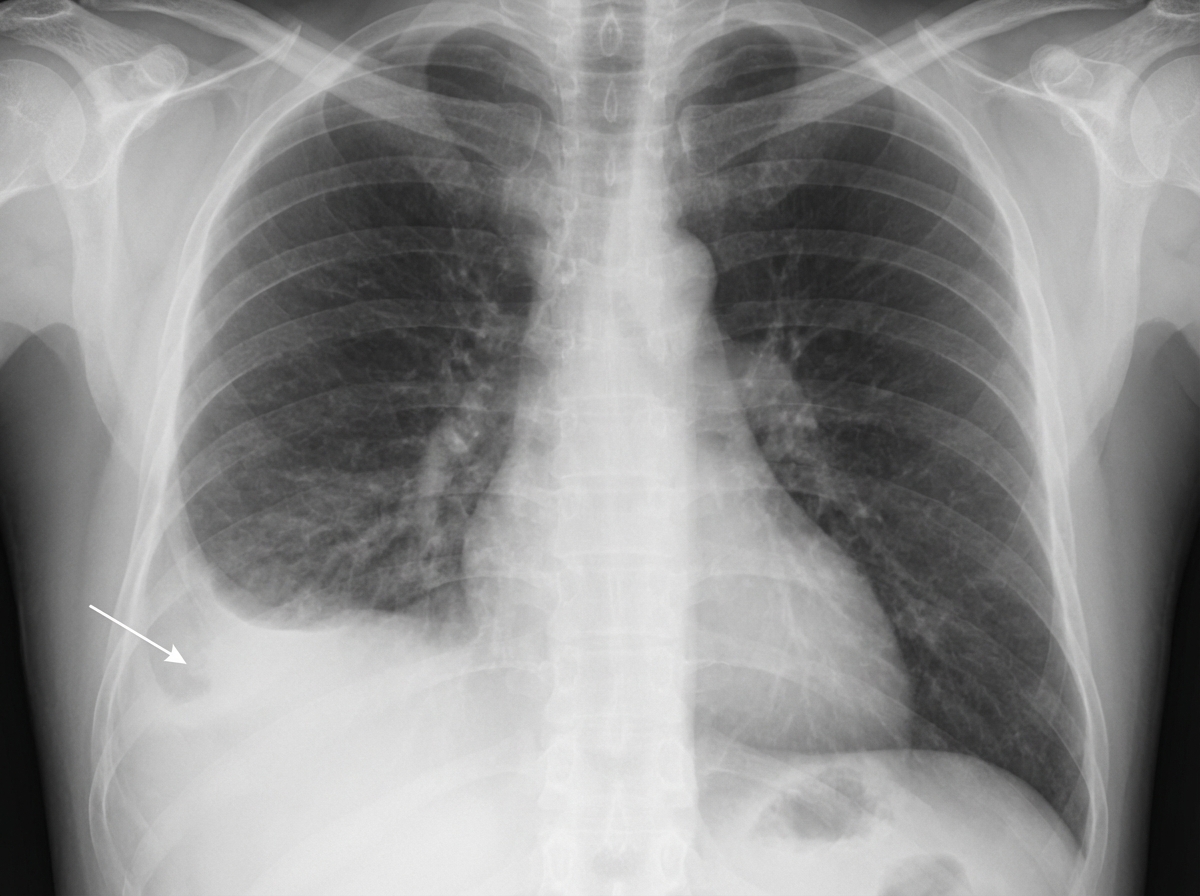
A patient with a known history of pulmonary tuberculosis presents to the emergency room with dyspnea. A chest X-ray reveals specific findings. Which of the following structures is NOT pierced during a diagnostic tap performed from the indicated structure?
Which of the following statements is true about the right atrium?
What artery supplies the SA node?
The thoracic duct terminates by emptying into which structure?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app