
Thorax — MCQs

On this page
A 45-year-old woman presents with severe dyspnea. Radiographic examination reveals a Pancoast tumor. Physical examination shows miosis of the pupil, partial ptosis of the eyelid, and facial anhydrosis. Which of the following structures has most likely been injured?
Which of the following is NOT true about the right phrenic nerve?
A patient presents with chest pain due to aspiration pneumonitis. On examination, there is dullness on percussion in the area medial to the medial border of the scapula on elevation of the arm. Which part of the lung is most likely to be affected?
What is true about the coronary sinus?
Which of the following statements about the SA node is incorrect?
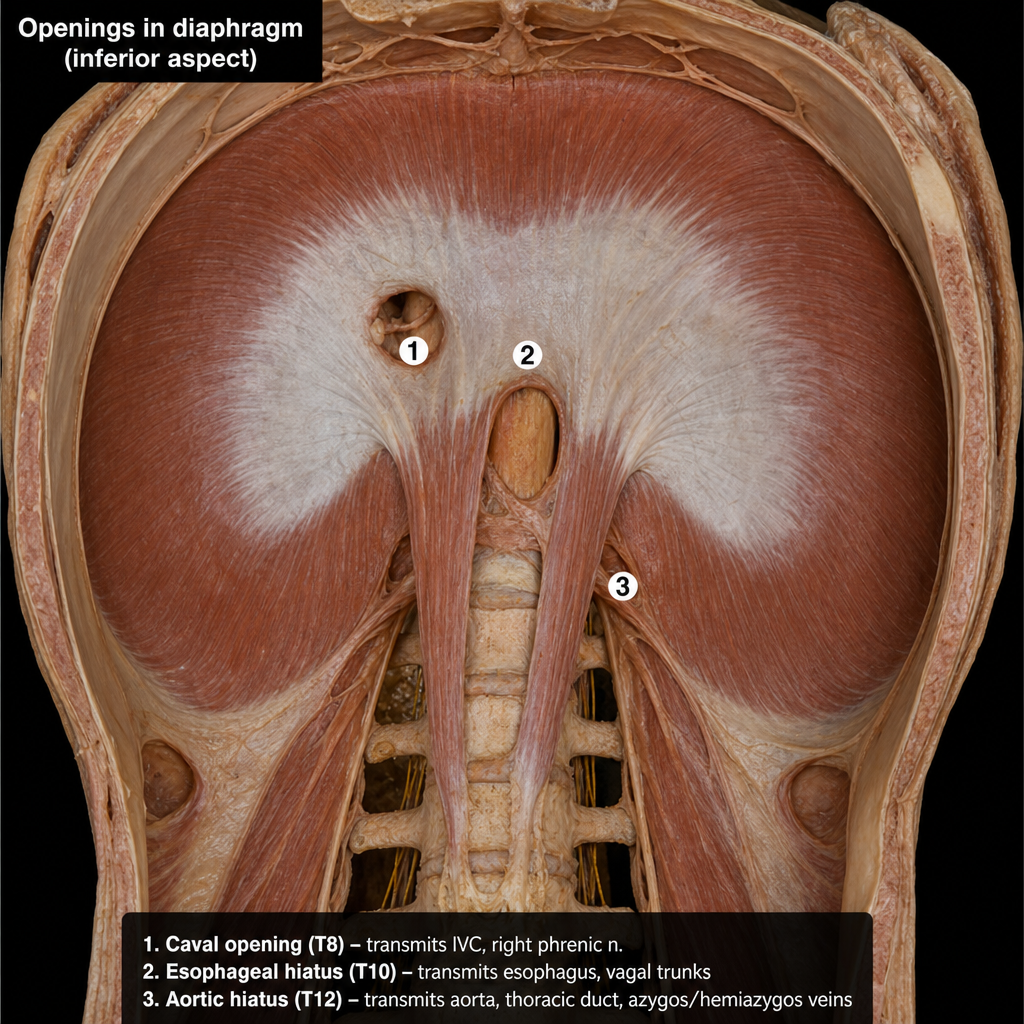
Which structure passes through the opening marked 3 in the diaphragm?
All of the following are true about coronary arteries, EXCEPT?
The third constriction of the esophagus is at the level of which anatomical landmark?
The triangle of Koch is bound by all of the following except?
Which of the following statements about the esophageal hiatus is TRUE?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app