
Thorax — MCQs

On this page
A 40-year-old male underwent coronary artery bypass grafting. During the procedure, the surgeon applied a clamp to the vessel lying anterior to the transverse pericardial sinus. Identify this vessel.
Which of the following statements regarding the diaphragm is true?
A 35-year-old female patient presents with a hard nodule approximately 1 cm in diameter, located slightly above and lateral to her right areola. A dye is injected into the tissue around the tumor, and lymphatic vessels draining the area are exposed by incision. These vessels, which uptake the visible dye, are traced to surgically expose the lymph nodes receiving lymph from the tumor. Which of the following lymph nodes will most likely first receive lymph drainage from this tumor?
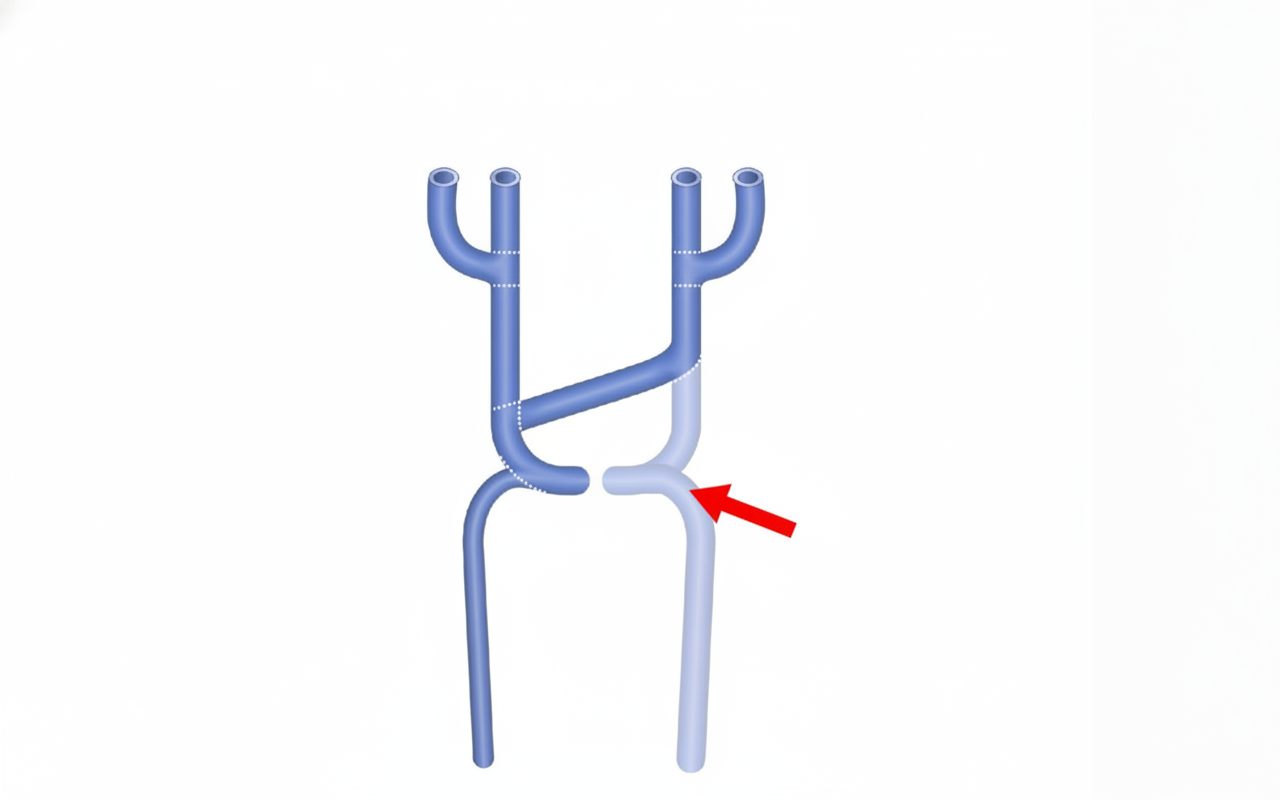
The arrow-marked structure drains into which chamber of the heart?
The left recurrent laryngeal nerve recurs around which structure?
What type of joint is the manubriosternal joint?
The deep cardiac plexus is located at which anatomical landmark?
Symptoms of thoracic outlet syndrome are produced due to compression of which nerve roots?
Which of the following is NOT a lobe of the lung?
Poirier's triangle is bound by all of the following except:
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app