
Thorax — MCQs

On this page
Which of the following represents the commonest variation in the arteries arising from the arch of the aorta?
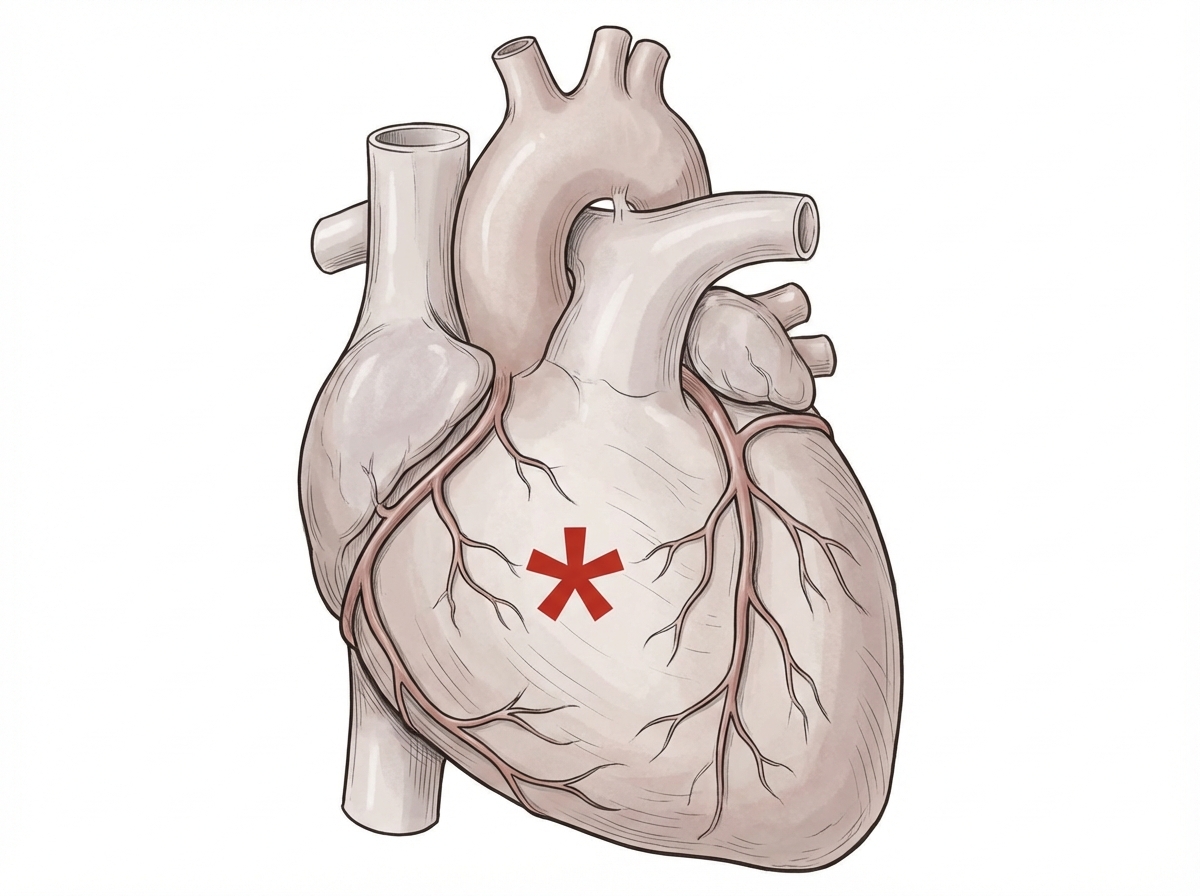
All of the following are arteries that supply the marked part of the specimen, except:
The right coronary artery supplies all of the following parts of the conducting system in the heart except?
Which structure does not pass through the esophageal hiatus?
All of the following vessels end directly in the right atrium except?
In the erect posture, what is the most common site for a foreign body in the bronchus?
Chylothorax is defined as the presence of chyle within the pleural cavity. What substance does chyle primarily consist of?
The sternochondral joint is classified as which type of joint?
During cardiac surgery, the transverse pericardial sinus allows easy placement of a vascular clamp upon which of the following vessels?
What is the normal fluid level in the pericardial cavity?
Practice by Chapter
Thoracic Wall and Diaphragm
Practice Questions
Pleura and Lungs
Practice Questions
Mediastinum
Practice Questions
Heart and Pericardium
Practice Questions
Great Vessels and Azygos System
Practice Questions
Thoracic Duct and Lymphatics
Practice Questions
Autonomic Innervation
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Thoracic Imaging and Cross-sectional Anatomy
Practice Questions
Embryological Development of Thoracic Structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app