
Systemic Anatomy — MCQs

On this page
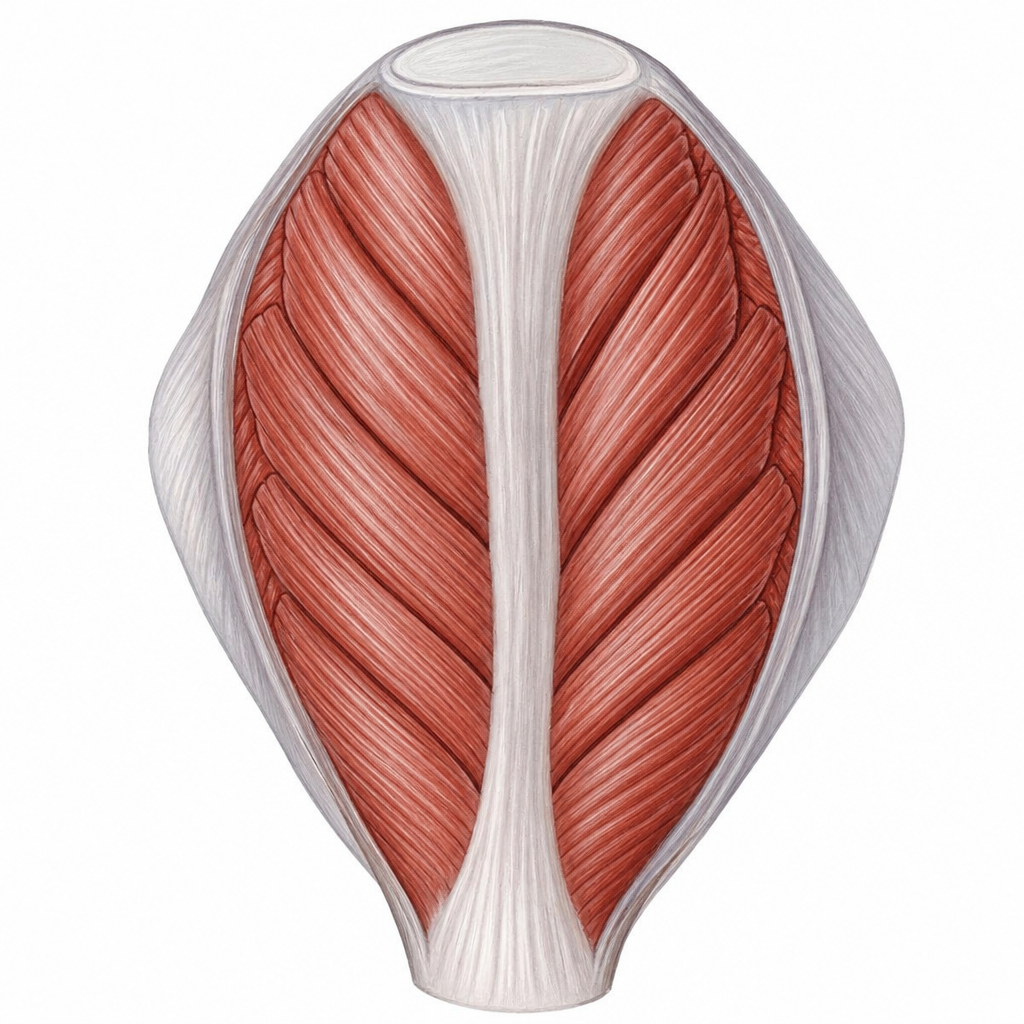
Identify the type of muscle shown in the image.
Which of the following is the most metabolically active part of long bone?
Food particles mostly get obstructed in which part of the esophagus?
Which of the following is a traction epiphysis?
Left recurrent laryngeal nerve passes between ?
Which of the following structures of joints is not innervated?
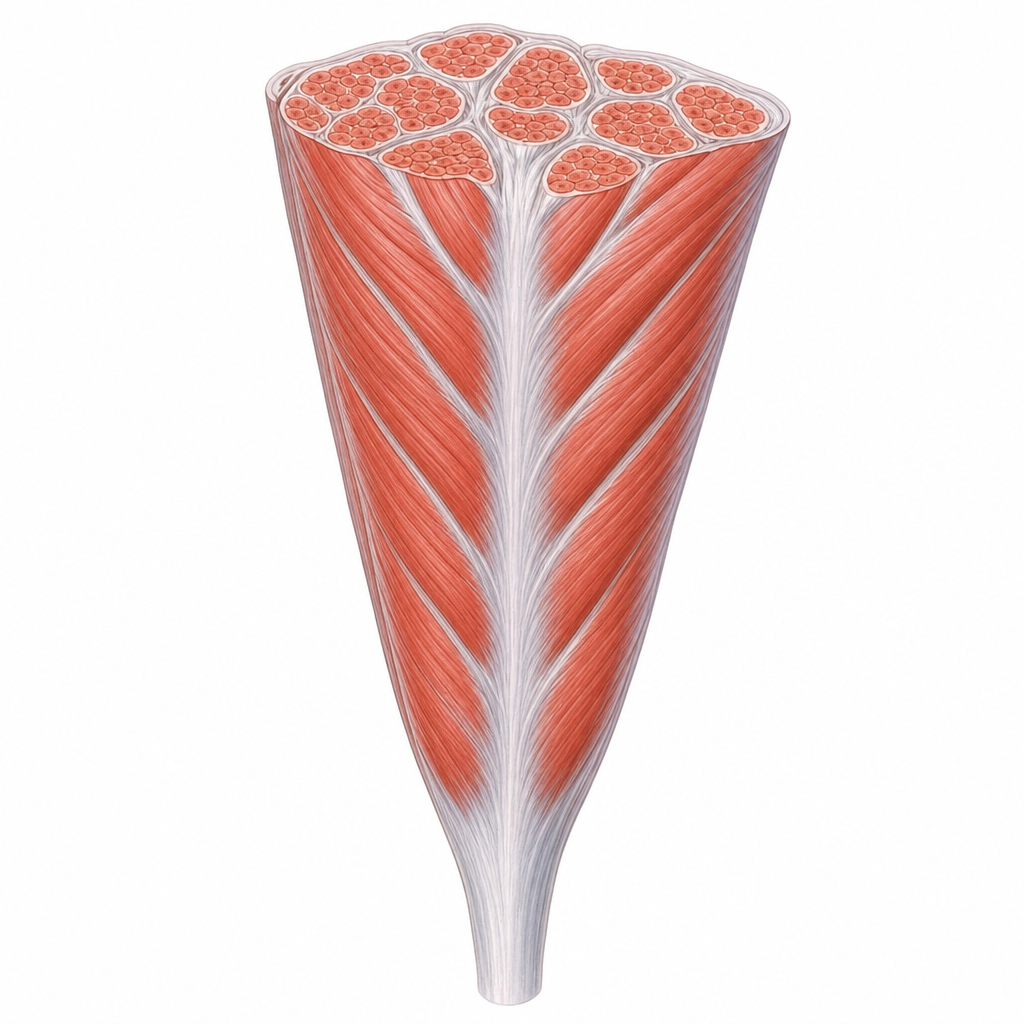
Identify the type of muscle shown in the image.
Which part of the bone is considered the most vascular zone?
Which organ receives dual blood supply with both sources contributing to its primary metabolic function?
Common hepatic artery is a branch of:
Practice by Chapter
Skeletal System
Practice Questions
Articular System
Practice Questions
Muscular System
Practice Questions
Cardiovascular System
Practice Questions
Lymphatic System
Practice Questions
Nervous System
Practice Questions
Respiratory System
Practice Questions
Digestive System
Practice Questions
Urinary System
Practice Questions
Reproductive System
Practice Questions
Endocrine System
Practice Questions
Integumentary System
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app