
Systemic Anatomy — MCQs

On this page
Greatest movement is seen in which type of joint?
A non-synovial joint with interosseous ligaments or fibrous connective tissue that allows slight movement is:
The connection of two bony structures with a ligament is known as
Joint between epiphysis and diaphysis of a long bone is a type of -
The location of Schatzki's ring is
Sclera is weakest at the level of:
Blood is supplied to bone from which arteries?
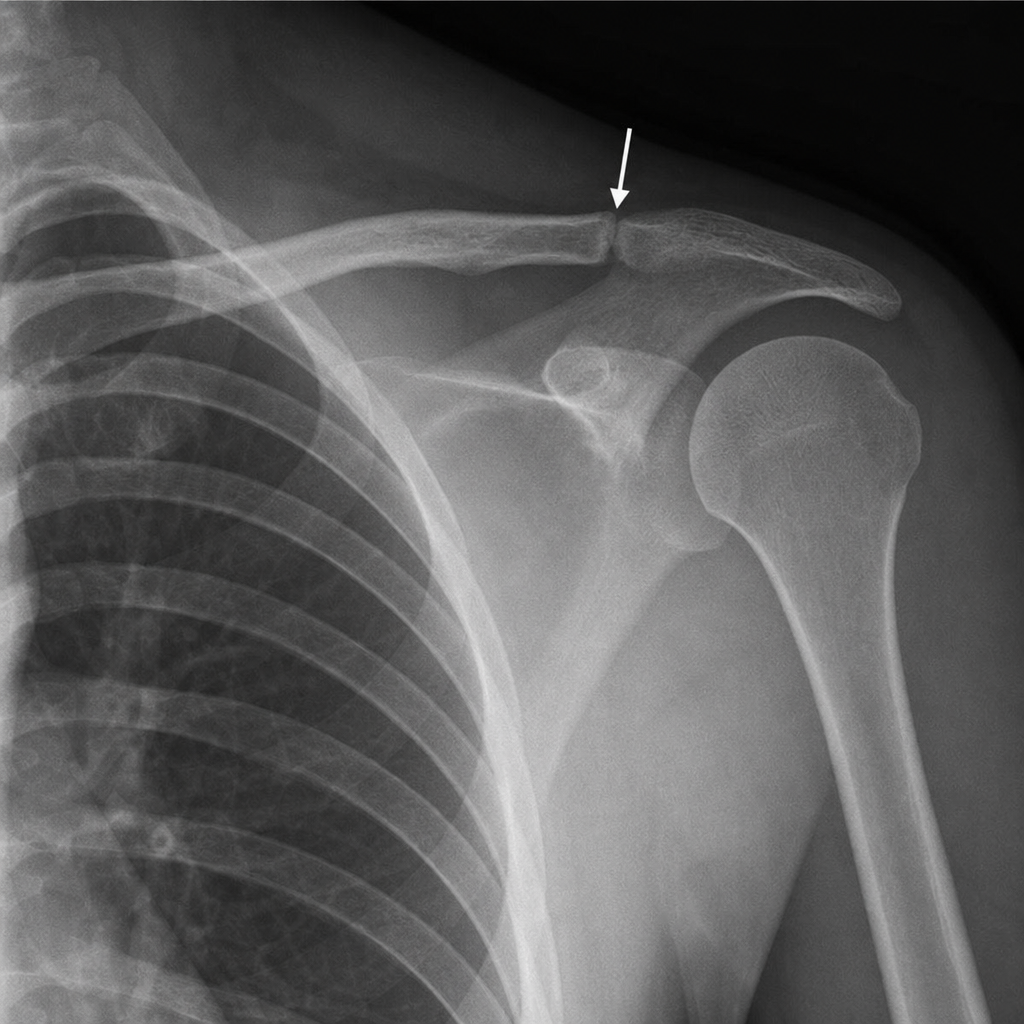
Type of joint at site marked by the arrow?
What anatomical feature of the lymphatic system is primarily responsible for filtering pathogens from lymph?
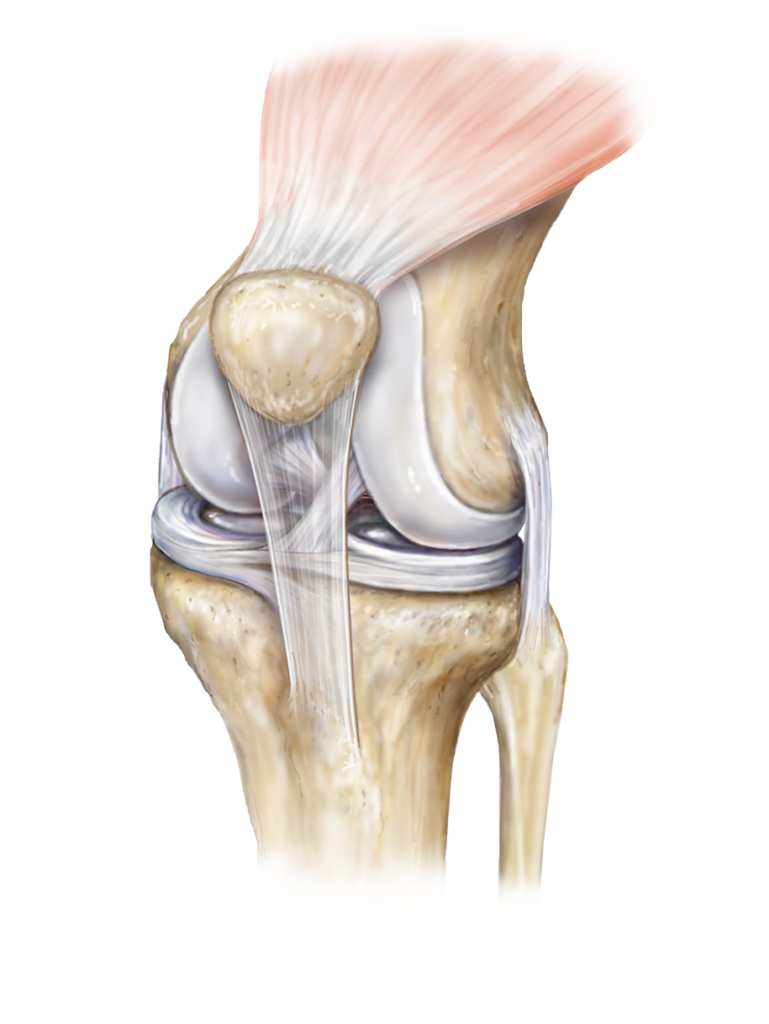
Identify the type of joint in the image provided.
Practice by Chapter
Skeletal System
Practice Questions
Articular System
Practice Questions
Muscular System
Practice Questions
Cardiovascular System
Practice Questions
Lymphatic System
Practice Questions
Nervous System
Practice Questions
Respiratory System
Practice Questions
Digestive System
Practice Questions
Urinary System
Practice Questions
Reproductive System
Practice Questions
Endocrine System
Practice Questions
Integumentary System
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app