
Systemic Anatomy — MCQs

On this page
Bones are held by a long cord or sheet of dense fibrous connective tissue called:
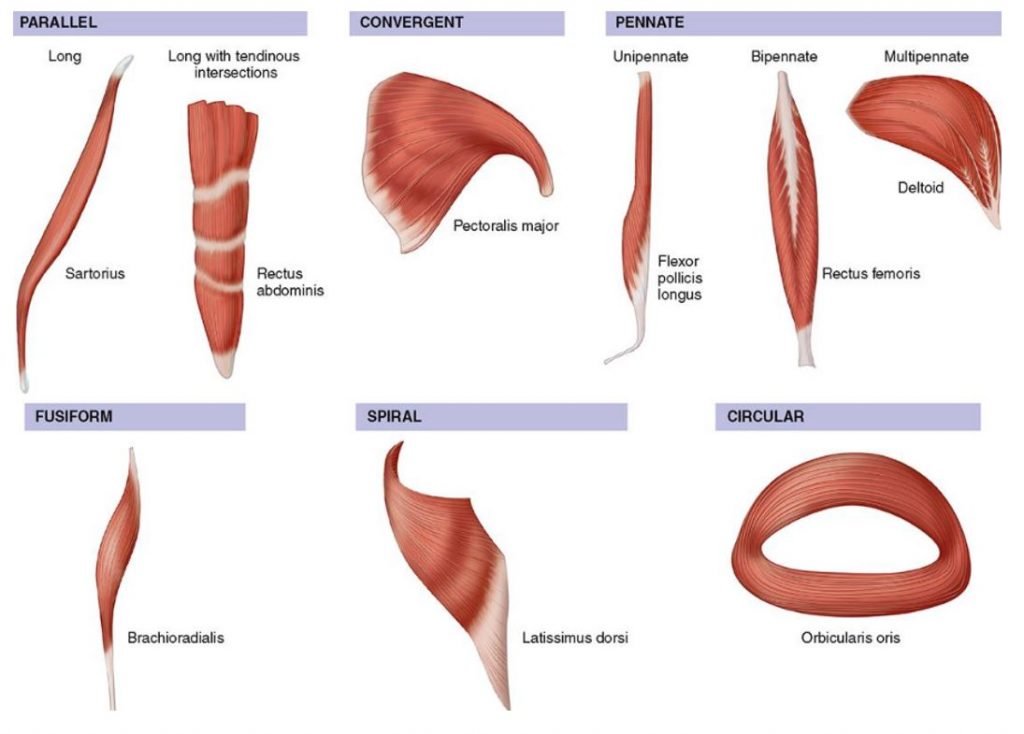
The muscle shown in the image is an example of which of the following type of muscle fiber arrangement?
Which is not a fibrous joint:
All of the following muscles have dual nerve supply, EXCEPT?
All are fibrous joints except:
Which of the following is NOT a hybrid muscle?
Hardest bone of the body is?
The largest organ of the body is:
Which of the following is an atavistic epiphysis?
Which is a hinge joint :
Practice by Chapter
Skeletal System
Practice Questions
Articular System
Practice Questions
Muscular System
Practice Questions
Cardiovascular System
Practice Questions
Lymphatic System
Practice Questions
Nervous System
Practice Questions
Respiratory System
Practice Questions
Digestive System
Practice Questions
Urinary System
Practice Questions
Reproductive System
Practice Questions
Endocrine System
Practice Questions
Integumentary System
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app