
Systemic Anatomy — MCQs

On this page
Which muscle does not have a dual nerve supply?
Small bones are supplied by which type of vessels?
Which of the following is NOT an end artery?
Which is the most vascular part of a bone?
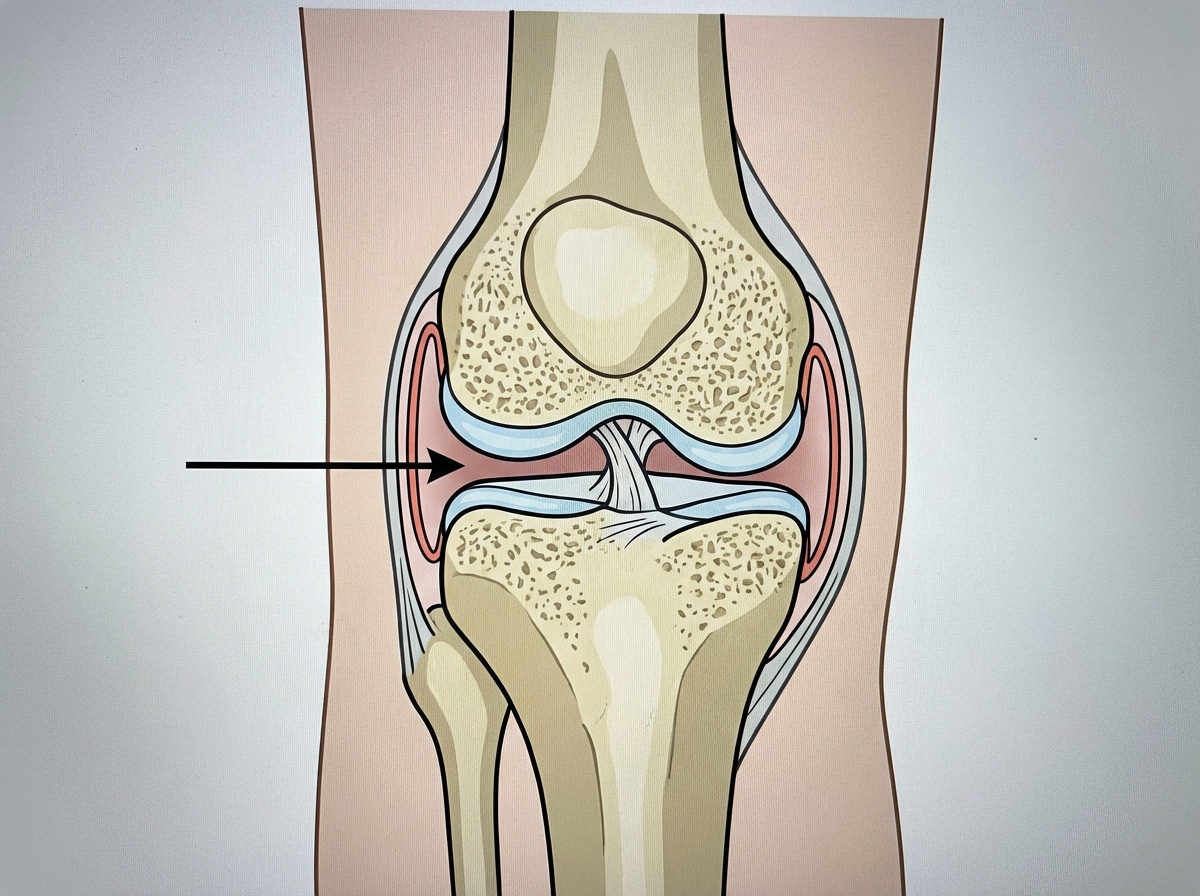
What type of joint is indicated at the site marked by the arrow?
All of the following organs are categorized as secondary lymphoid organs, EXCEPT?
All of the following joints ossify by 16 years of age except?
Which of the following statements concerning the circulatory system is true?
Vertebral arteries are derived from:
Which of the following muscles is NOT part of the digastric group?
Practice by Chapter
Skeletal System
Practice Questions
Articular System
Practice Questions
Muscular System
Practice Questions
Cardiovascular System
Practice Questions
Lymphatic System
Practice Questions
Nervous System
Practice Questions
Respiratory System
Practice Questions
Digestive System
Practice Questions
Urinary System
Practice Questions
Reproductive System
Practice Questions
Endocrine System
Practice Questions
Integumentary System
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app