
Surface and Radiological Anatomy — MCQs

On this page
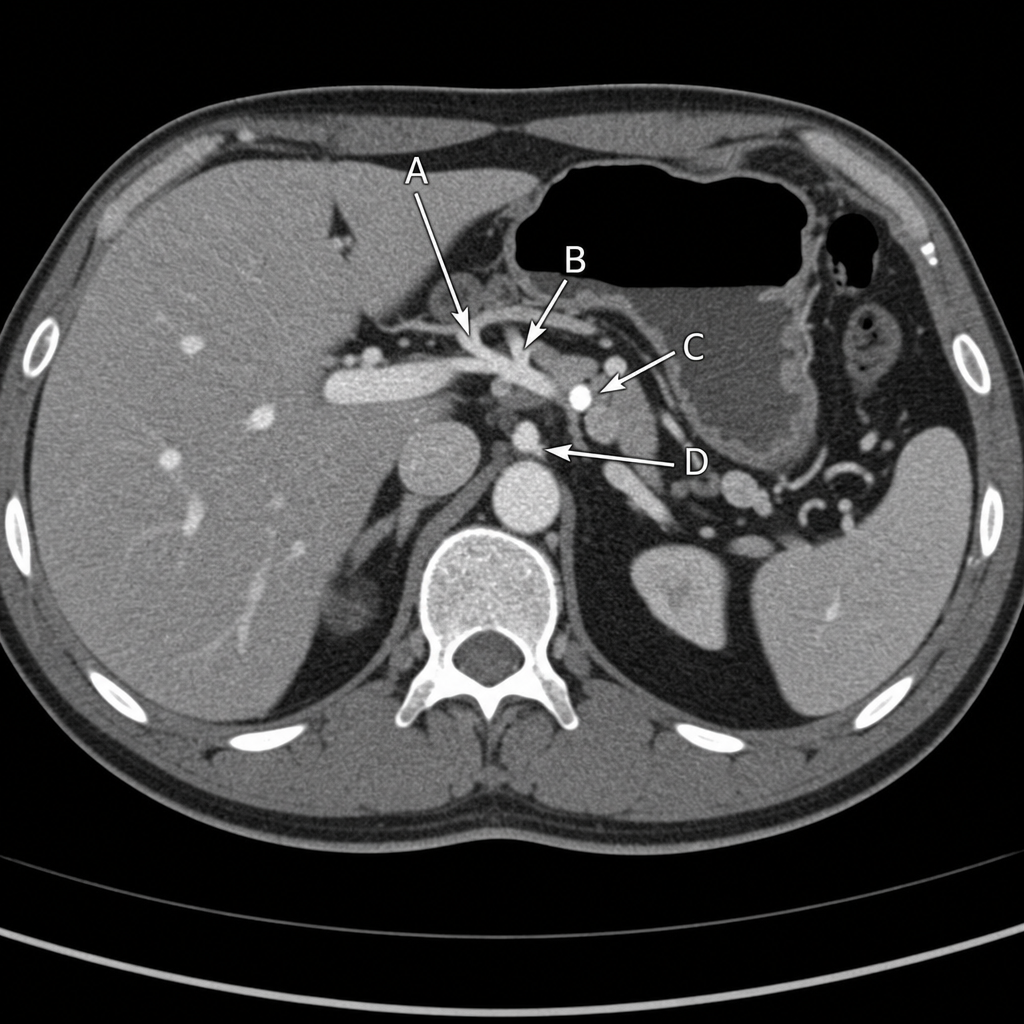
Which structure, as identified in the provided CT scan of the abdomen at the level of the 12th thoracic vertebra, is divided into the proper hepatic and gastroduodenal arteries?
The tip of the T3 spinous process corresponds to which anatomical landmark?
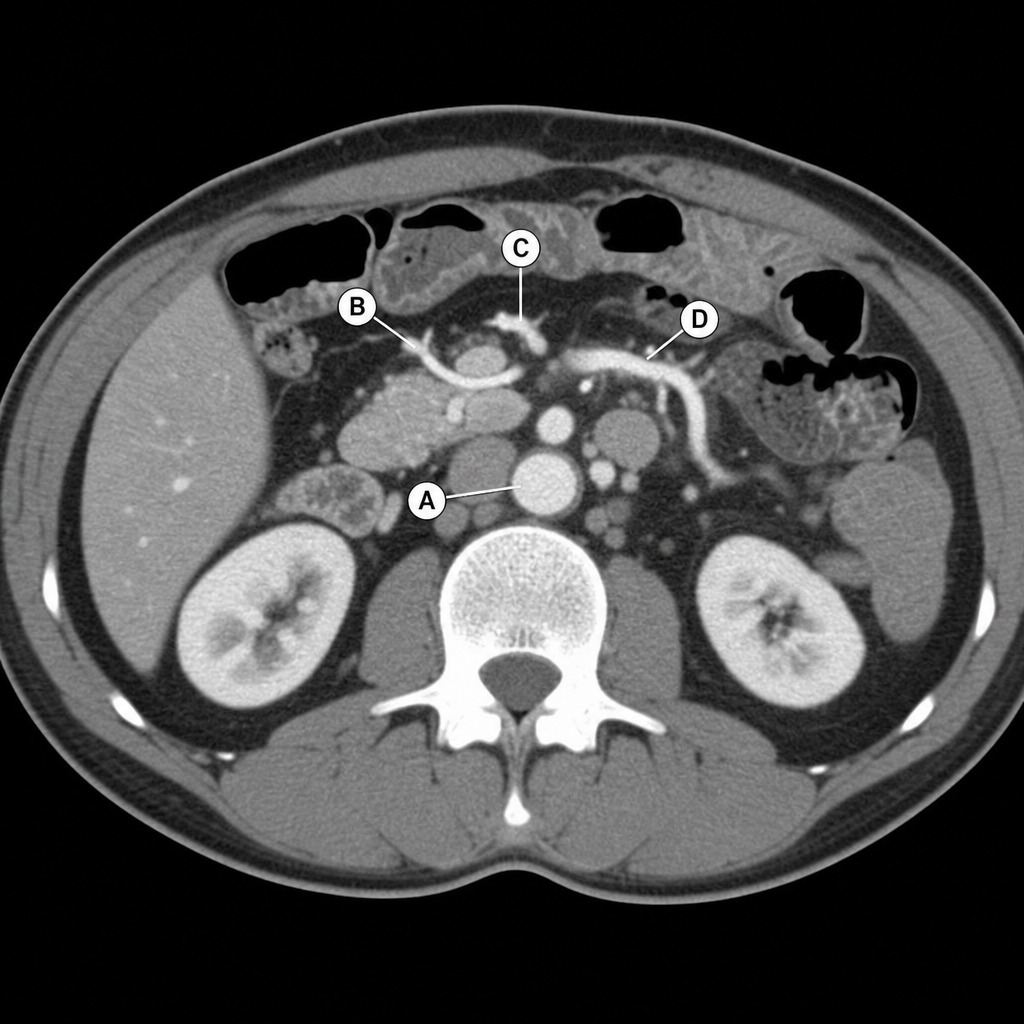
On a CT scan of the abdomen at the level of the upper lumbar vertebrae, which structure is a direct branch of the aorta and supplies blood to the ascending and transverse colons?
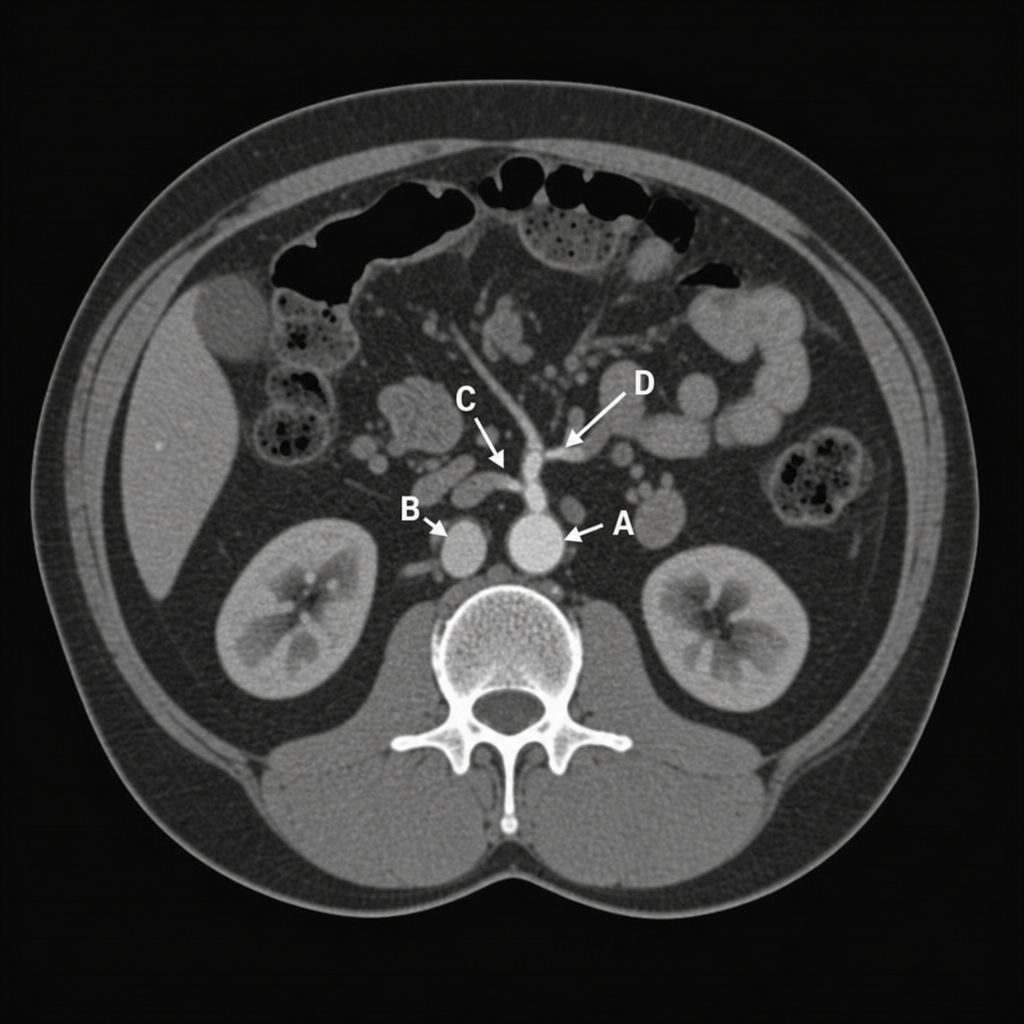
In this CT scan of the abdomen at the level of the upper lumbar vertebra, which structure is a direct branch of the aorta and supplies blood to the ascending and transverse colons?
A 30-year-old male presented to the emergency department after suffering a stab wound over the anterior chest wall in the left midclavicular line. CT scan revealed a penetrating injury through the lower border of the left lung. At which rib level is the wound most likely located?
A 54-year-old female is admitted to the hospital with a stab wound of the thoracic wall in the area of the right fourth costal cartilage. Which of the following pulmonary structures is present at this site?
What is the lamina dura?
Posterior superior iliac spine is at the level of which vertebral level?
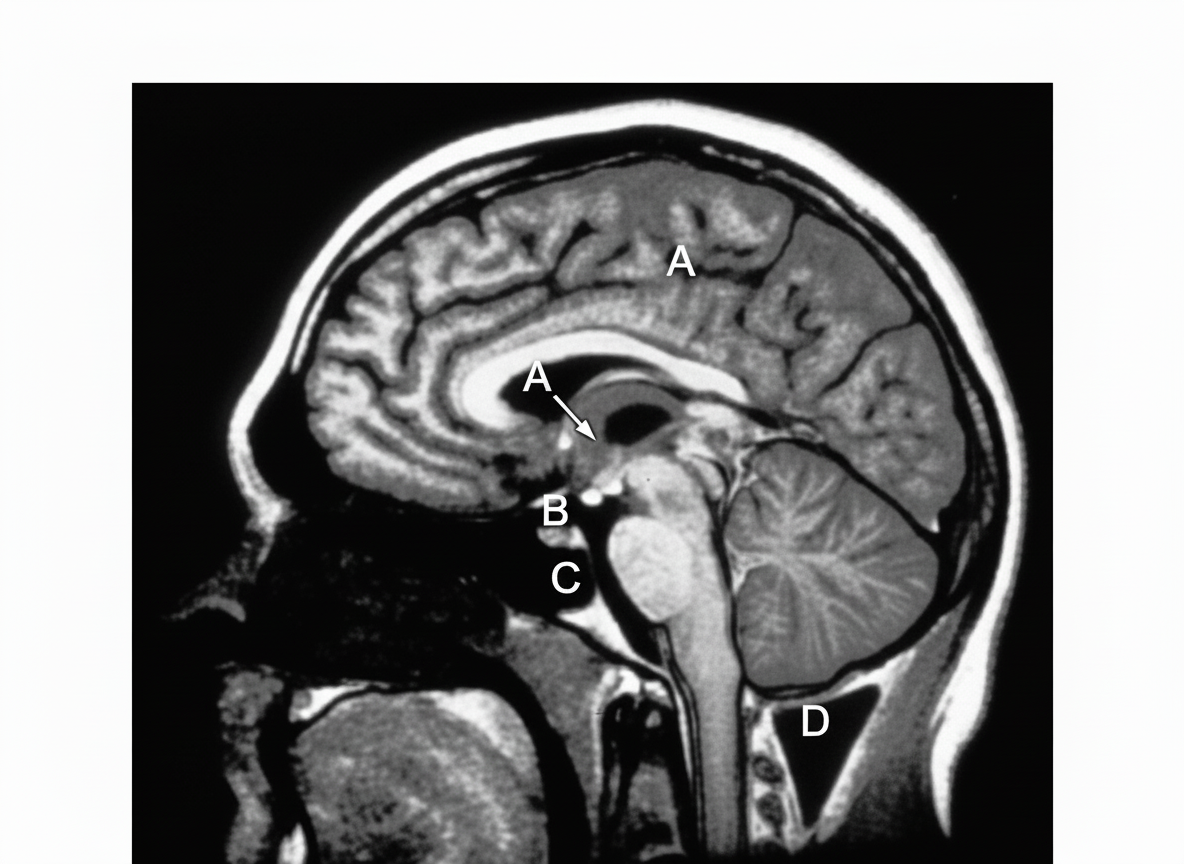
In the provided MRI scan showing a sagittal section through the head and neck, a tumor originating from which labeled structure can be surgically accessed via a transsphenoidal approach, passing through the nasal septum and the body of the sphenoid bone?
In a CT scan at the level of the celiac trunk, which of the following structures will be seen?
Practice by Chapter
Surface Landmarks of the Head and Neck
Practice Questions
Surface Landmarks of the Thorax
Practice Questions
Surface Landmarks of the Abdomen
Practice Questions
Surface Landmarks of the Limbs
Practice Questions
Radiographic Anatomy
Practice Questions
CT Anatomy
Practice Questions
MRI Anatomy
Practice Questions
Ultrasonographic Anatomy
Practice Questions
Angiographic Anatomy
Practice Questions
Sectional and Cross-sectional Anatomy
Practice Questions
Anatomical Correlations in Common Imaging
Practice Questions
Interventional Radiological Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app