
Microscopic Anatomy — MCQs

On this page
In which of the following organs are 'peg cells' characteristically seen?
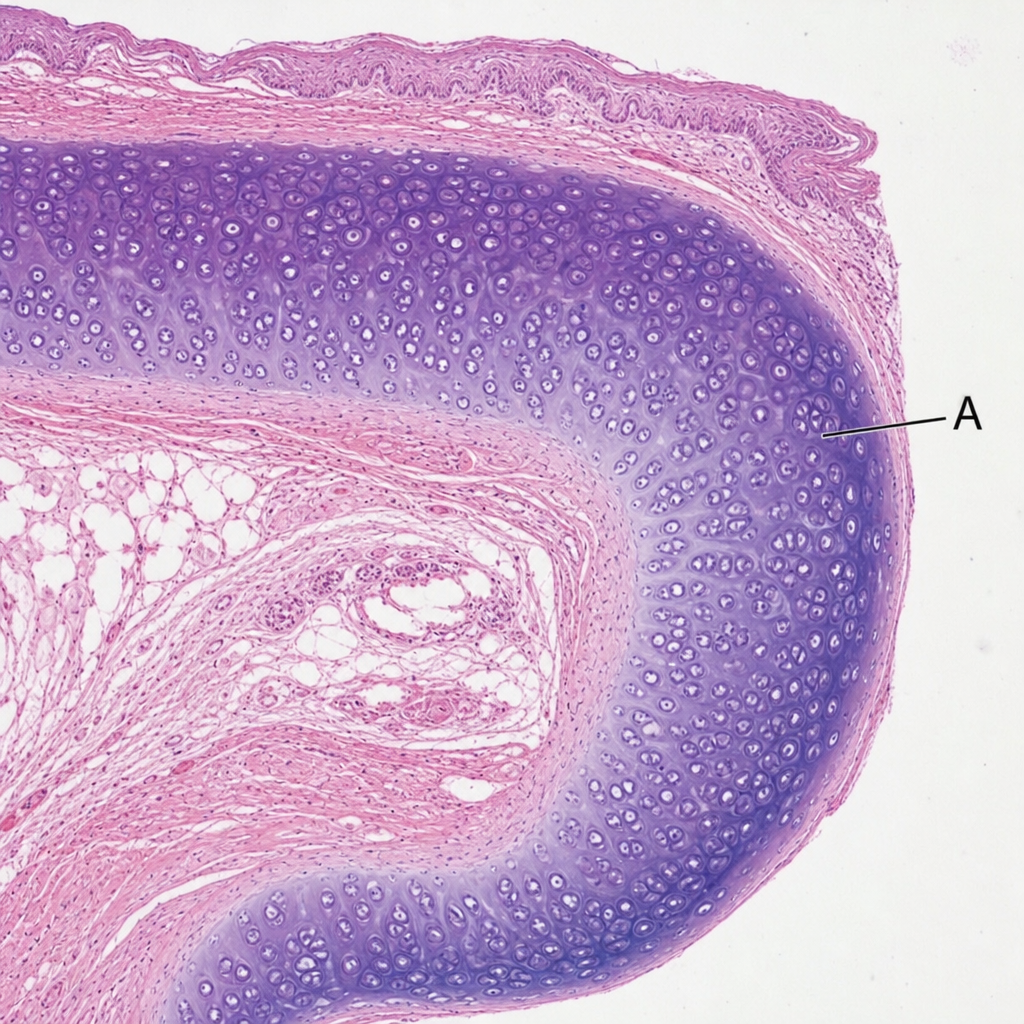
The cartilage of A is:
After maturation in the thymus and release into the circulation, T lymphocytes preferentially migrate to which of the following sites?
What is the epithelial lining of the vagina?
The ureter is lined by which type of epithelium?
What type of epithelium lines the proximal convoluted tubule (PCT)?
Which of the following is true about the stratum lucidum?
What is the epithelial lining of the glottis/true vocal cords?
In the intra-epithelial region of the mucosa of the intestine, what is the predominant cell population?
Which kidney epithelium has the most mitochondria per cell?
Practice by Chapter
Cellular Ultrastructure
Practice Questions
Microscopic Anatomy of Epithelial Tissues
Practice Questions
Microscopic Anatomy of Connective Tissues
Practice Questions
Microscopic Anatomy of Muscle Tissues
Practice Questions
Microscopic Anatomy of Nervous Tissues
Practice Questions
Microscopic Anatomy of Blood and Immune System
Practice Questions
Microscopic Anatomy of Endocrine Glands
Practice Questions
Microscopic Anatomy of Digestive System
Practice Questions
Microscopic Anatomy of Respiratory System
Practice Questions
Microscopic Anatomy of Urinary System
Practice Questions
Microscopic Anatomy of Reproductive System
Practice Questions
Techniques in Microscopic Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app