
Microscopic Anatomy — MCQs

On this page
Which banding technique is most commonly employed for cytogenetic analysis?
What is the approximate length of the distal convoluted tubule?
Which of the following statements about Brucella is false?
Hypersensitivity vasculitis usually involves which of the following structures?
Tight junctions are primarily located at which part of the cell?
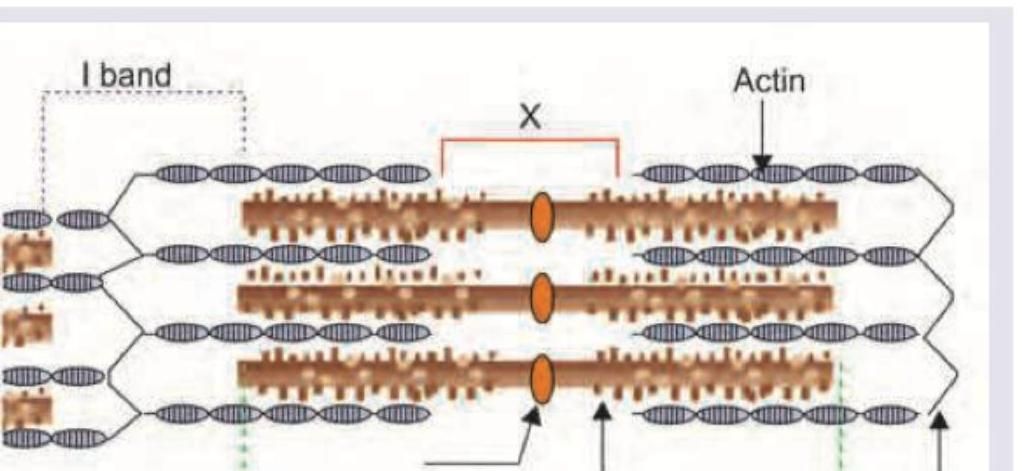
In the sarcomere diagram shown below, what do the marked areas X and Y represent?
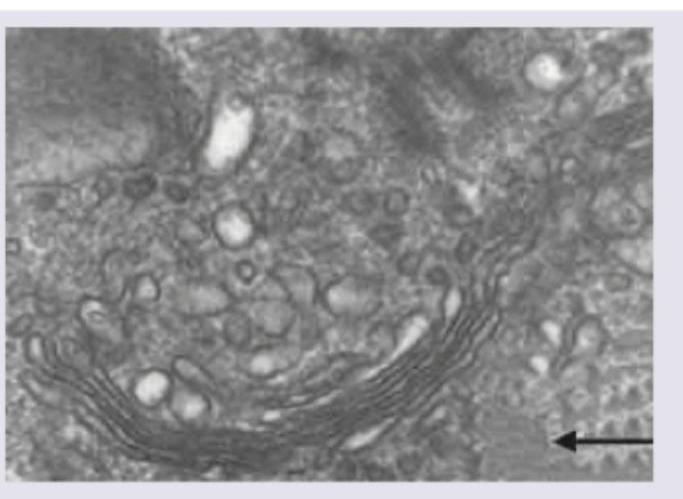
In this electron micrograph, identify the structure marked with arrow.
Which of the following proteins are not seen in the region marked in the image?
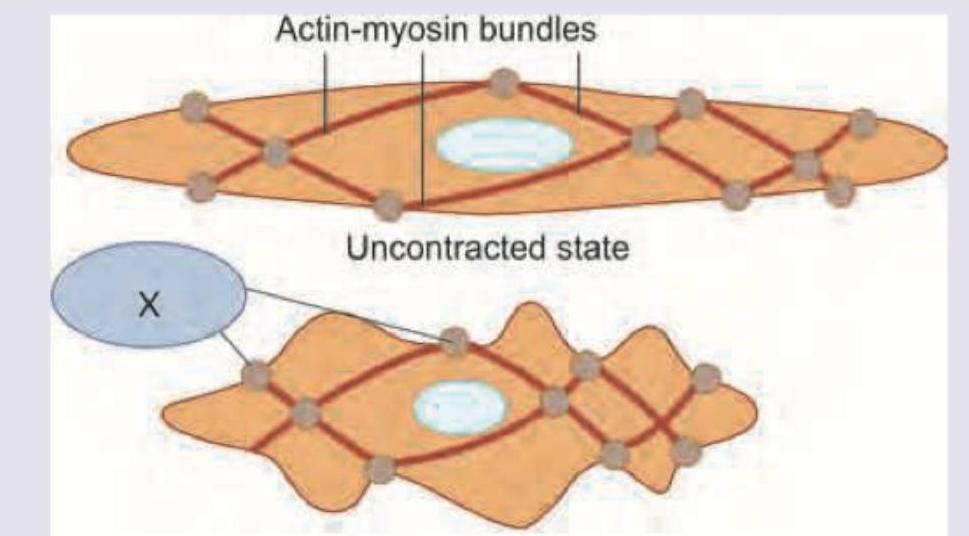
Which is correct about structures marked as "X" found in smooth muscle?
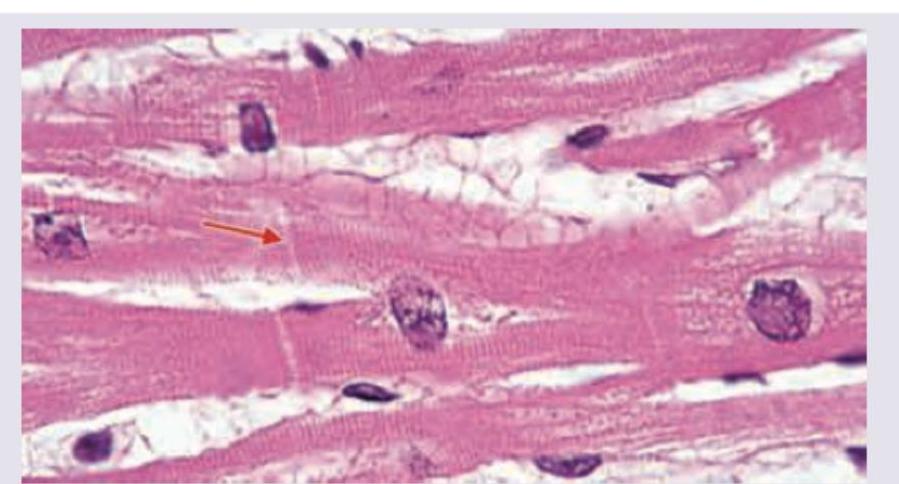
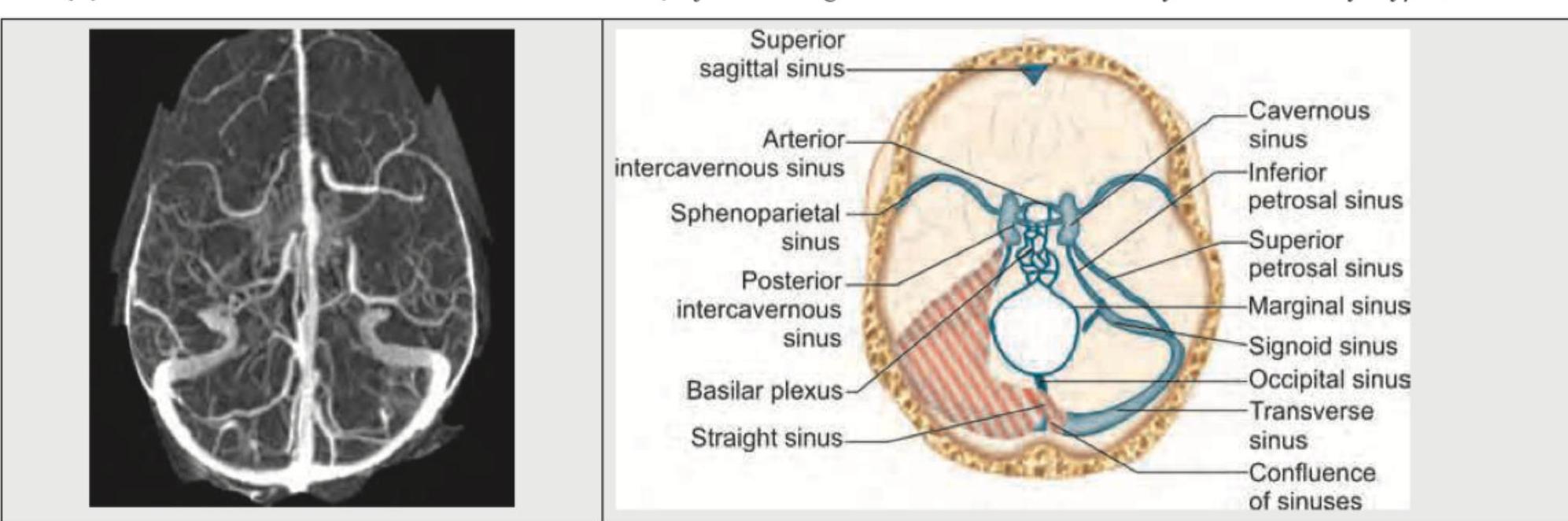
Identify the anatomical structure shown in the image.
Practice by Chapter
Cellular Ultrastructure
Practice Questions
Microscopic Anatomy of Epithelial Tissues
Practice Questions
Microscopic Anatomy of Connective Tissues
Practice Questions
Microscopic Anatomy of Muscle Tissues
Practice Questions
Microscopic Anatomy of Nervous Tissues
Practice Questions
Microscopic Anatomy of Blood and Immune System
Practice Questions
Microscopic Anatomy of Endocrine Glands
Practice Questions
Microscopic Anatomy of Digestive System
Practice Questions
Microscopic Anatomy of Respiratory System
Practice Questions
Microscopic Anatomy of Urinary System
Practice Questions
Microscopic Anatomy of Reproductive System
Practice Questions
Techniques in Microscopic Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app