
Clinical Anatomy — MCQs

On this page
Froment's sign (book test) is used to assess the function of adductor pollicis. Which of the following nerves supplies this muscle?
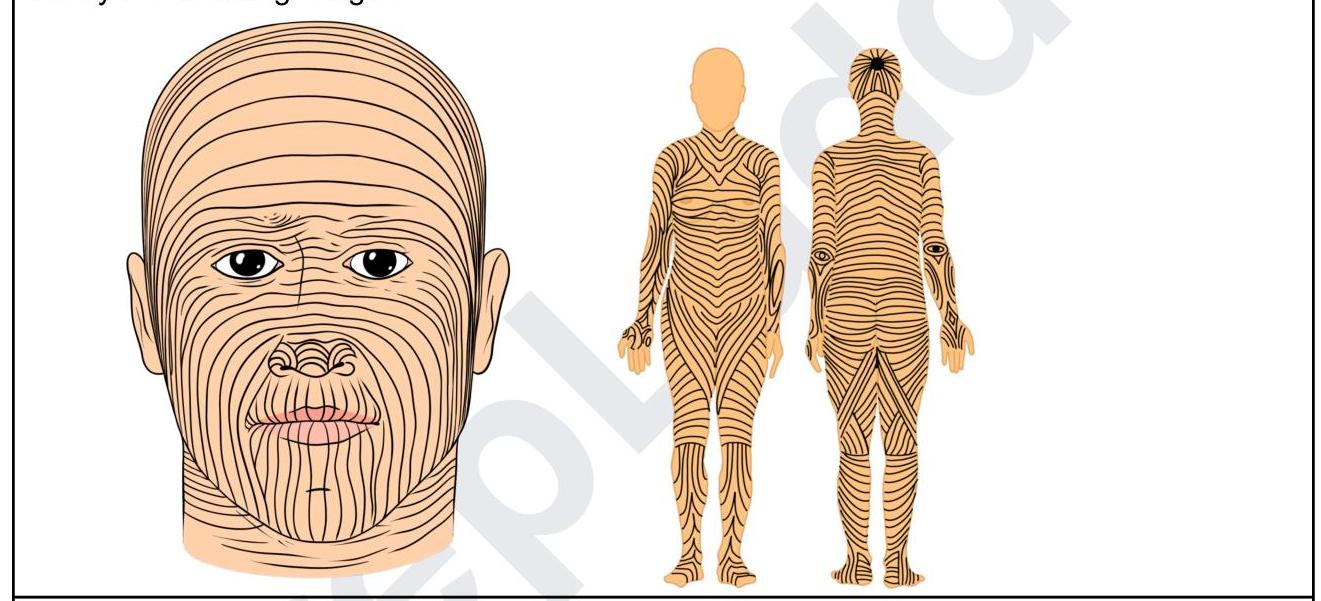
Identify the lines shown in the following image:
A patient after a road traffic accident presents to the emergency room with difficulty in swallowing and slurred speech. Investigations reveal fractures in the occipitotemporal region. Which of the following areas should be tested in order to find the nerve which is involved?
A patient who has taken the first COVID vaccine comes for the second dose. An astute nurse noticed that the shoulder was flabby, flat, and was asymmetrical. There was an associated loss of contour of the shoulder joint. Injury to which of the structures might have resulted and was avoidable?
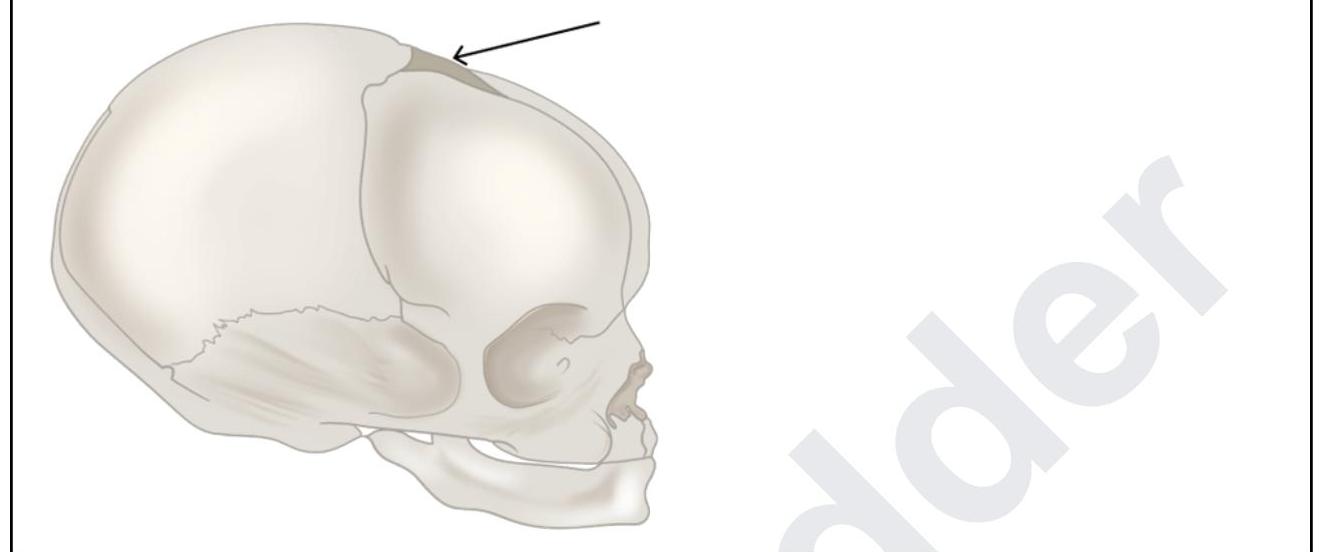
A 6-month-old boy was brought to the casualty with seizures. The pediatrician tries to do CSF sampling. What are the structures punctured by the pediatrician while piercing through the marked structure?
During a thyroidectomy, a surgeon must carefully identify and preserve the parathyroid glands. These glands are most commonly located posterior to which part of the thyroid gland?
An MRI of a patient with low back pain reveals compression of the L5 nerve root. Which of the following muscles would most likely show weakness during physical examination?
A 45-year-old woman undergoes a modified radical mastectomy for breast cancer. Following the procedure, she experiences numbness in the medial aspect of her upper arm. Which of the following nerves was most likely injured during the surgery?
In which location is a transplanted kidney typically placed?
Winging of scapula is due to paralysis of
Practice by Chapter
Anatomical Basis of Common Clinical Conditions
Practice Questions
Surgical Anatomy
Practice Questions
Anatomical Basis of Trauma
Practice Questions
Anatomical Aspects of Infections
Practice Questions
Anatomical Considerations in Regional Anesthesia
Practice Questions
Anatomical Basis of Physical Examination
Practice Questions
Clinical Correlations in Neuroanatomy
Practice Questions
Anatomical Approaches in Minimally Invasive Procedures
Practice Questions
Imaging Correlations in Clinical Anatomy
Practice Questions
Anatomical Variations of Clinical Importance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app