
Clinical Anatomy — MCQs

On this page
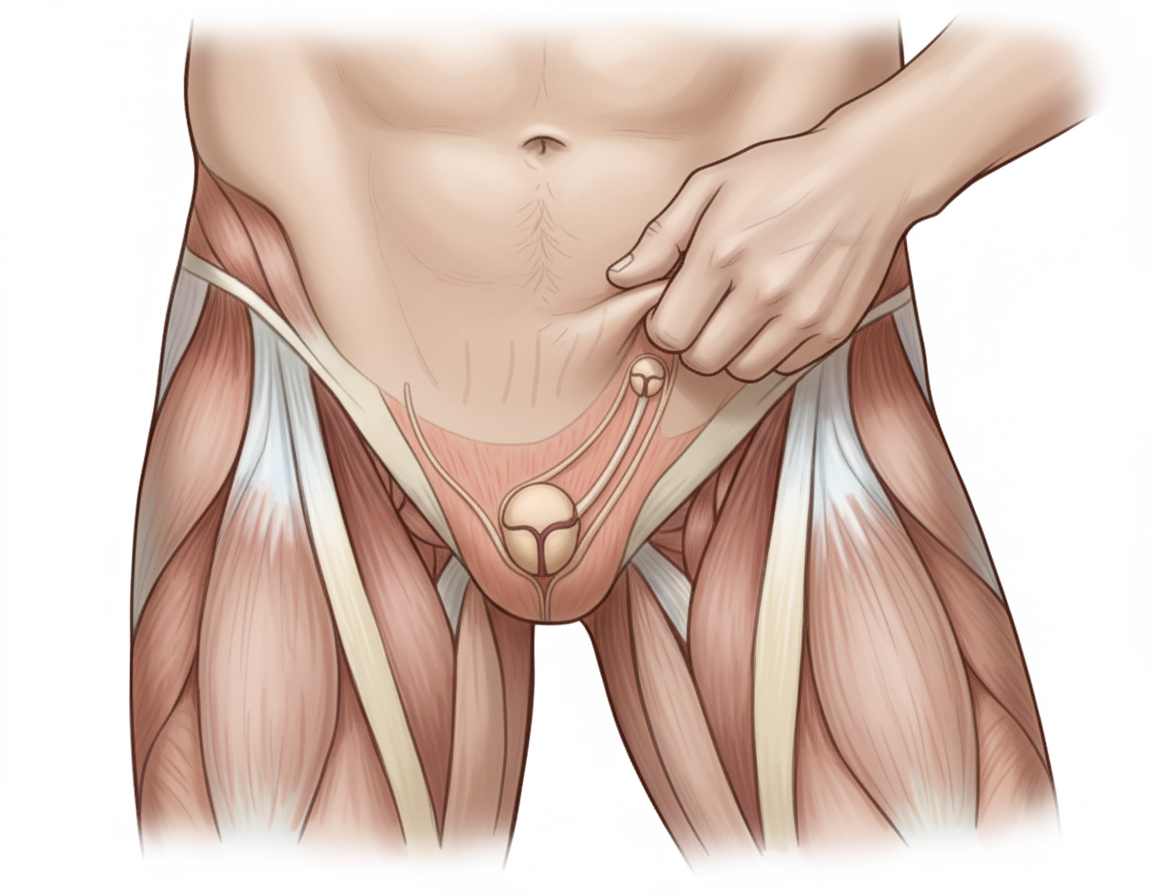
The image shows performance of the Cremasteric Reflex with ipsilateral elevation of testis. Which nerve mediates this reflex? Additional information: - Afferent: Femoral branch of genitofemoral nerve - Efferent: Genital branch of genitofemoral nerve - The reflex is elicited by lightly stroking the skin on the medial aspect of the superior part of the thigh - Rapid elevation of the testis on the same side confirms the cremasteric reflex - This reflex is extremely active in children
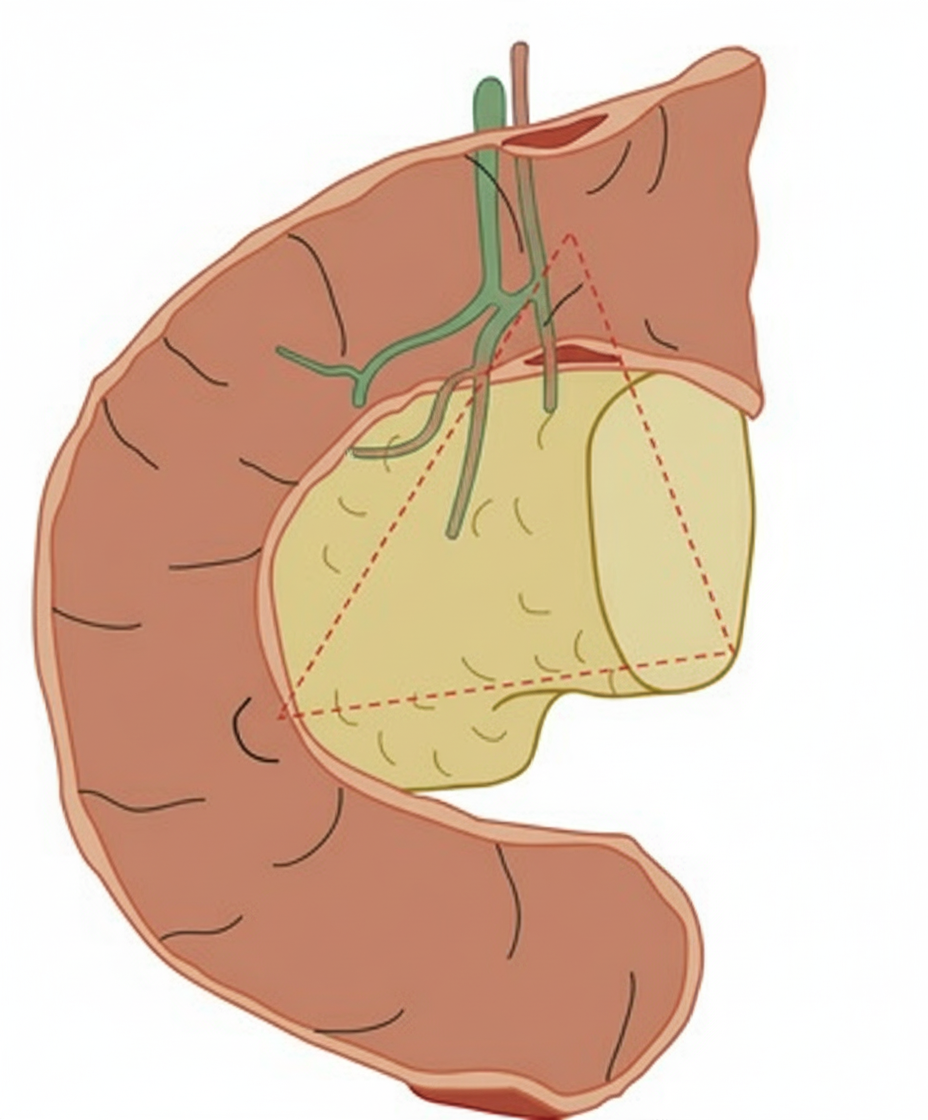
The image shows a triangular anatomical region with the following boundaries: 1. Confluence of cystic duct with common hepatic duct 2. Junction of head and body of pancreas 3. Junction of second and third parts of duodenum. Identify the structure:
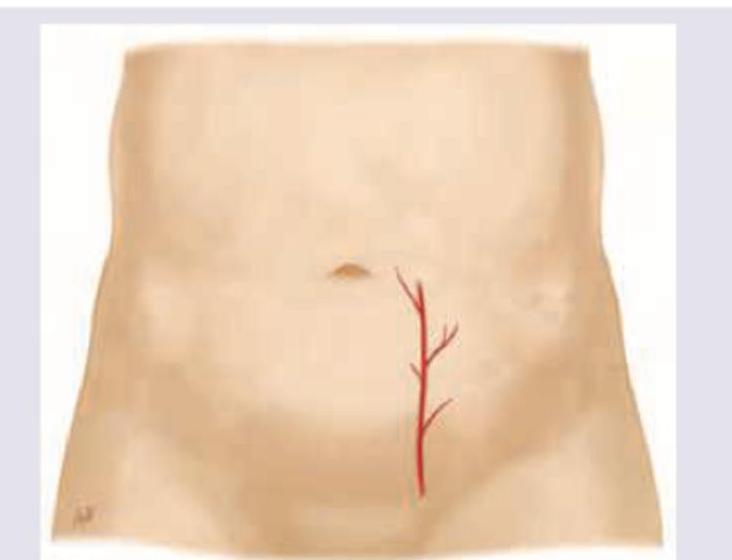
Which artery shown here should be avoided during paracentesis?
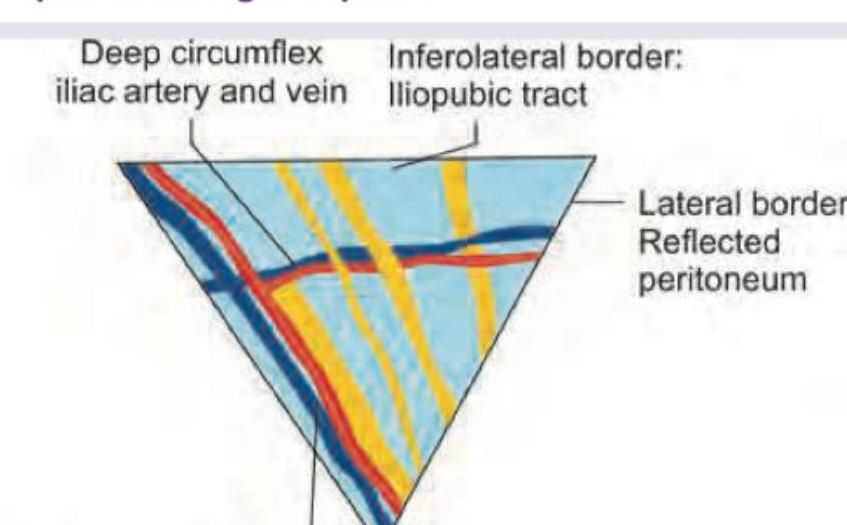
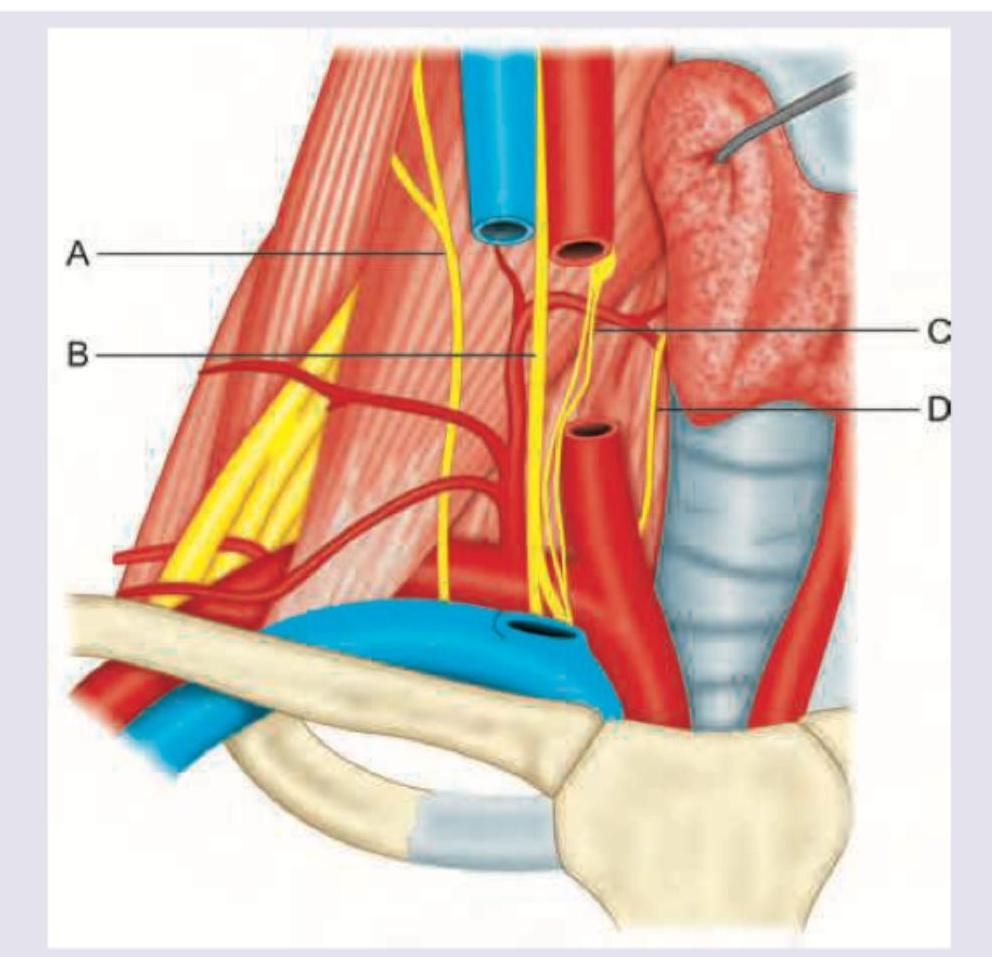
Which of the nerves shown in yellow color is not a part of the triangle of pain?
In this diagram, identify the structure whose paralysis causes decrease in respiratory movements: (AIIMS May 2016)
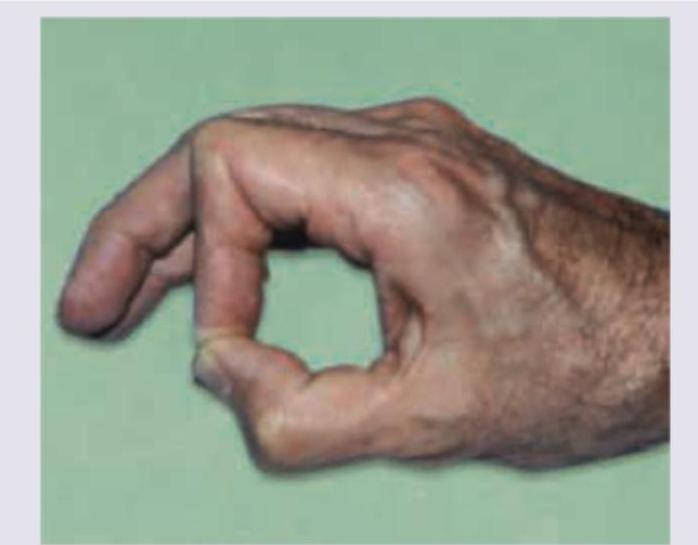
Identify the nerve damaged in the picture:
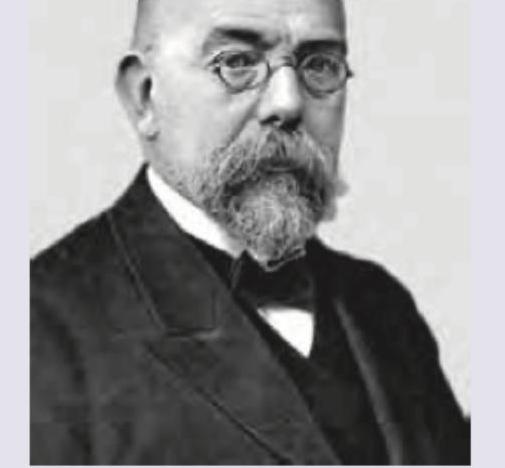
Identify the scientist. (Recent NEET Pattern 2016-17)
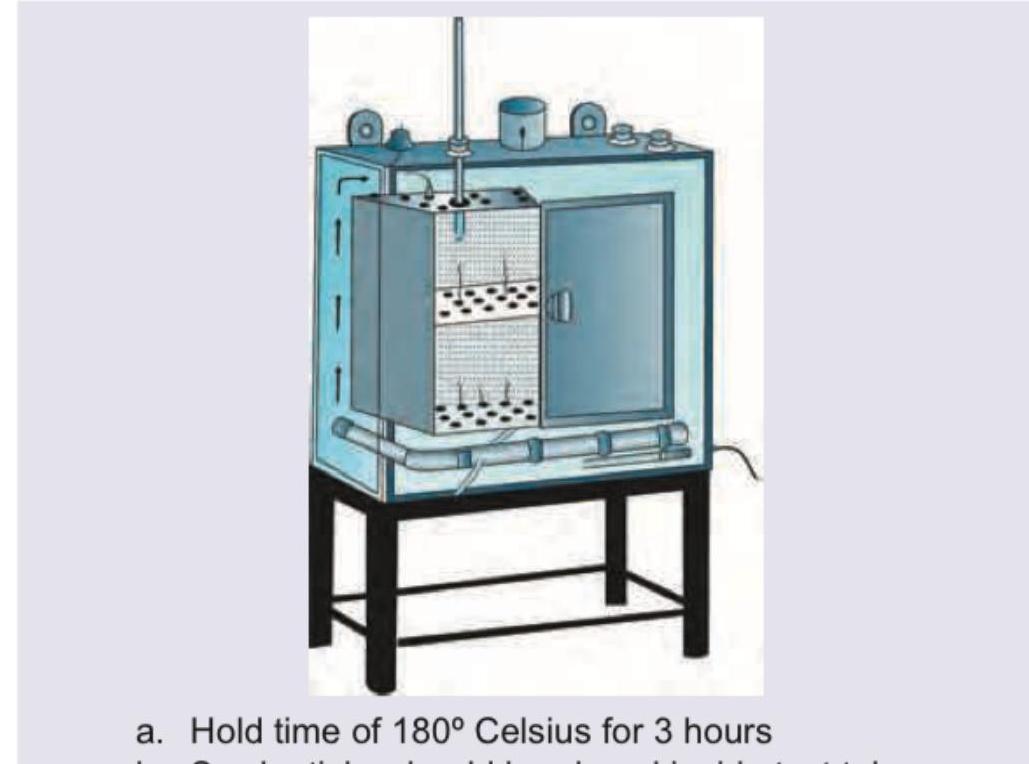
The following instrument is sterilized using:

The suture material shown below is sterilized by which method?

All are correct about the method of sterilization shown here except:
Practice by Chapter
Anatomical Basis of Common Clinical Conditions
Practice Questions
Surgical Anatomy
Practice Questions
Anatomical Basis of Trauma
Practice Questions
Anatomical Aspects of Infections
Practice Questions
Anatomical Considerations in Regional Anesthesia
Practice Questions
Anatomical Basis of Physical Examination
Practice Questions
Clinical Correlations in Neuroanatomy
Practice Questions
Anatomical Approaches in Minimally Invasive Procedures
Practice Questions
Imaging Correlations in Clinical Anatomy
Practice Questions
Anatomical Variations of Clinical Importance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app