
Clinical Anatomy — MCQs

On this page
Garlicky odor in the gastric contents is characteristic of which non-metallic poisoning?
A patient presented to OPD with ophthalmoplegia and ptosis. Diagnosis of superior orbital fissure syndrome was confirmed after examination. Which nerves are compressed in this case ?
Which of the following veins is involved in the formation of esophageal varices?
A woman presents with a breast lump, associated with skin dimpling and nipple retraction. What is the most likely anatomical structure responsible for the skin dimpling?
A patient presents with loss of sensation on the posterior surface of the ear along with a lesion. Which structure is most likely involved?
A 55-year-old man is diagnosed with left testicular carcinoma. Which of the following lymph nodes is the first to be involved?
A patient presented to the OPD with an abnormal gait. On examination, a right-sided hip drop was observed when the patient was asked to stand on the left foot. Which of the following muscles are paralyzed in this patient?
A middle-aged lady choked while eating fish and has associated symptoms of coughing, hoarseness of voice, and a foreign body sensation in the throat. On examination, the pyriform fossa is found to be inflamed. Which of the following nerves supplies this region?
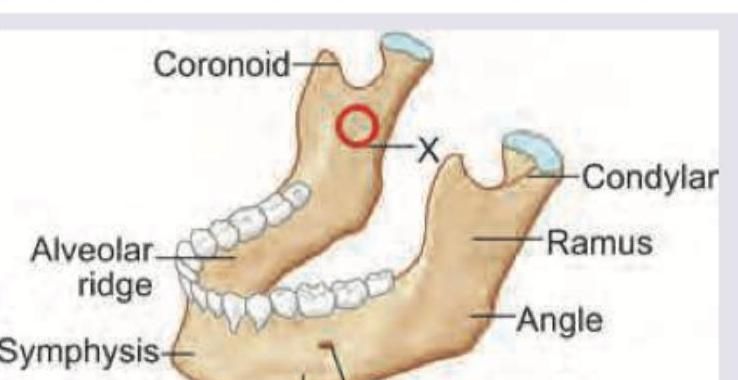
While giving inferior alveolar block, the injection is given above which foramen marked as X ?
All of the following sites are used for the route of adrenaline administration shown below except:

Practice by Chapter
Anatomical Basis of Common Clinical Conditions
Practice Questions
Surgical Anatomy
Practice Questions
Anatomical Basis of Trauma
Practice Questions
Anatomical Aspects of Infections
Practice Questions
Anatomical Considerations in Regional Anesthesia
Practice Questions
Anatomical Basis of Physical Examination
Practice Questions
Clinical Correlations in Neuroanatomy
Practice Questions
Anatomical Approaches in Minimally Invasive Procedures
Practice Questions
Imaging Correlations in Clinical Anatomy
Practice Questions
Anatomical Variations of Clinical Importance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app