All (227)Anatomy (7)Biochemistry (2)Community Medicine (59)Dermatology (1)ENT (1)General Medicine (2)Internal Medicine (21)Microbiology (5)Obstetrics and Gynecology (66)Ophthalmology (2)Orthopaedics (2)Pathology (10)Pediatrics (5)Pharmacology (2)Physiology (8)Radiology (5)Surgery (29)
Q91
The ratio between incidences among exposed and non-exposed persons is called
Q92
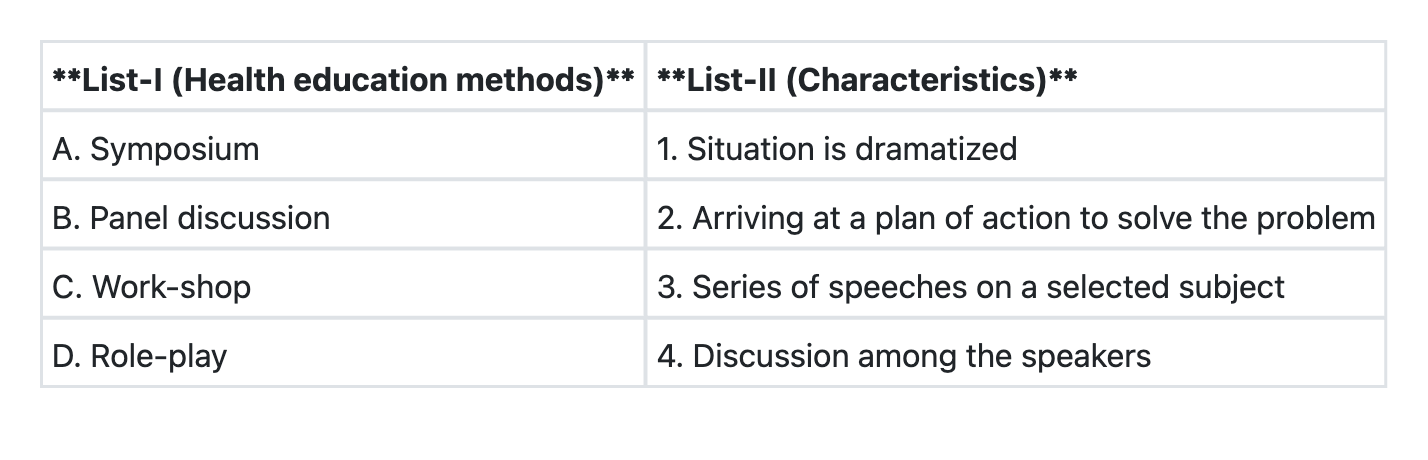
Match List-I with List-II and select the correct answer using the code given below the Lists:
Q93
A new drug is to be evaluated for its therapeutic effect. The best study design will be.
Q94
Consider the following criteria for a "screening test" : 1. Disease should have a latent period 2. Condition (disease) should be rare 3. Disease should be amenable to treatment Which of the above must be satisfied before including a screening test into any programme?
Q95
"Risk ratio" is also known as:
Q96
Consider the following characteristics of biological agents : 1. Infectivity 2. Pathogenicity 3. Virulence 4. Communicability Among the above characteristics, which are used to measure the ability of biological agents to induce clinically apparent illness?
Q97
"Mid-year population" is not the denominator of which mortality rate?
Q98
The best indicator for the measurement of "completed family size"; that is the number of children a woman would have through her reproductive years is
Q99
Under the DOTS strategy of Revised National Tuberculosis Programme, the recommended line of management in Category I patients, if the sputum is positive after 2 months of Intensive Phase treatment with 4 drugs, is to