All (107)Anatomy (2)Anesthesiology (3)Community Medicine (32)Internal Medicine (8)Microbiology (1)Obstetrics and Gynecology (29)Pathology (3)Pediatrics (5)Pharmacology (2)Physiology (2)Radiology (1)Surgery (19)
Q71
After male sterilization, additional contraceptive protection is
Q72
The life expectancy at birth for a country A is 64 years. The minimum and maximum values of life expectancy are 20 years and 86 years respectively. As part of Human Development Index (HDI), what is the Life Expectancy Index for the country A ?
Q73
Which of the following indicators stand consolidated in Physical Quality of Life Index (PQLI)? 1. Infant mortality 2. Life expectancy at age one 3. Per capita income 4. Literacy
Q74
Consider the following staff: 1. Medical Officer 2. Pharmacist 3. Anaesthetist 4. Health Educator Of them, who are routinely posted to a PHC ?
Q75
Which one of the following management techniques helps in standardising the methods of performing jobs ?
Q76
STDs are transmitted by
Q77
In which one of the following study designs, the unit of study involves populations rather than individuals ?
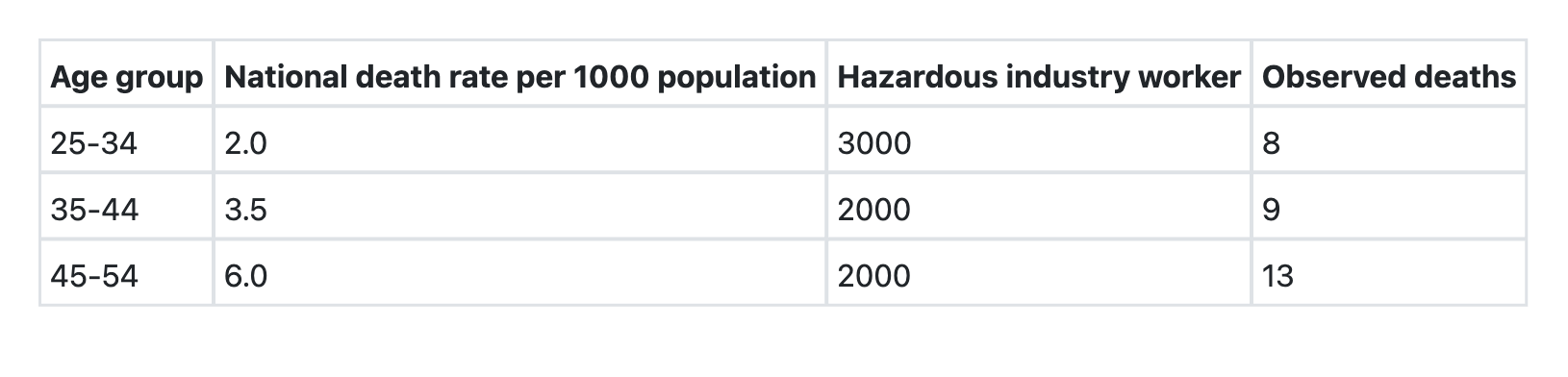
Q78
What is the Standardized Mortality Ratio (SMR) for the hazardous industry workers (as compared to national population)?
Q79
Which one of the following best explains the relationship among Prevalence (P), Incidence (I) and Duration (D) of a disease given the assumption that the population is stable ?