UPSC-CMS 2021 — Community Medicine
27 Previous Year Questions with Answers & Explanations
As per ICMR guidelines, which of the following are the criteria for SARS-COV-2 exposure for a pregnant female during the COVID-19 pandemic? 1. Travel to an affected country within previous 14 days 2. Close contact with a confirmed case within a distance of 1 metre for more than 15 minutes 3. Residing in a containment zone 4. Healthcare workers examining a confirmed case without adequate protection
Steroidal contraceptives available in the basket of contraceptive choice from Ministry of Health & Family Welfare, Government of India are
The life expectancy at birth for a country A is 64 years. The minimum and maximum values of life expectancy are 20 years and 86 years respectively. As part of Human Development Index (HDI), what is the Life Expectancy Index for the country A ?
Which of the following indicators stand consolidated in Physical Quality of Life Index (PQLI)? 1. Infant mortality 2. Life expectancy at age one 3. Per capita income 4. Literacy
Consider the following staff: 1. Medical Officer 2. Pharmacist 3. Anaesthetist 4. Health Educator Of them, who are routinely posted to a PHC ?
Which one of the following management techniques helps in standardising the methods of performing jobs ?
STDs are transmitted by
In which one of the following study designs, the unit of study involves populations rather than individuals ?
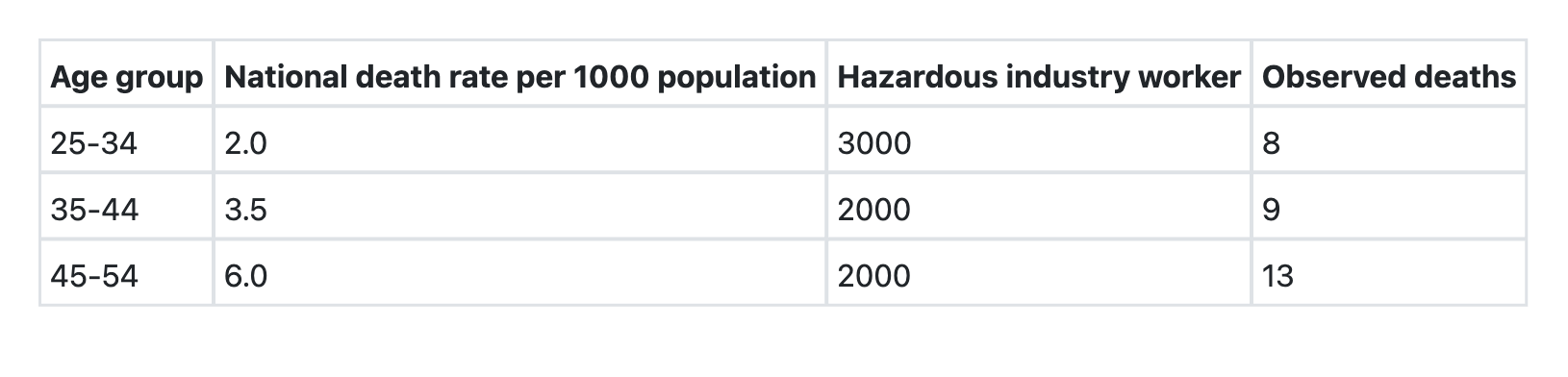
What is the Standardized Mortality Ratio (SMR) for the hazardous industry workers (as compared to national population)?
Which one of the following best explains the relationship among Prevalence (P), Incidence (I) and Duration (D) of a disease given the assumption that the population is stable ?
UPSC-CMS 2021 - Community Medicine UPSC-CMS Practice Questions and MCQs
Question 1: As per ICMR guidelines, which of the following are the criteria for SARS-COV-2 exposure for a pregnant female during the COVID-19 pandemic? 1. Travel to an affected country within previous 14 days 2. Close contact with a confirmed case within a distance of 1 metre for more than 15 minutes 3. Residing in a containment zone 4. Healthcare workers examining a confirmed case without adequate protection
- A. 1, 2 and 3
- B. 1, 2 and 4 (Correct Answer)
- C. 1, 3 and 4
- D. 2, 3 and 4
Explanation: ***1, 2 and 4*** - As per **ICMR guidelines for COVID-19 exposure assessment**, the criteria for direct SARS-CoV-2 exposure included: - **Travel to an affected country** within the previous 14 days (epidemiological link) - **Close contact with a confirmed case** (within 1 meter for more than 15 minutes without adequate protection) - **Healthcare workers examining confirmed cases** without adequate personal protective equipment - These represent **direct exposure pathways** requiring immediate testing and quarantine protocols for pregnant women. *1, 2 and 3* - While travel history and close contact are valid direct exposure criteria, **residing in a containment zone** represents an **area-based epidemiological risk factor** rather than a direct exposure event. - Containment zone residence warranted enhanced surveillance but did not constitute direct exposure unless accompanied by specific contact history or symptoms. - This option incorrectly omits criterion 4 (healthcare workers without protection), which was a critical direct occupational exposure pathway. *1, 3 and 4* - This option incorrectly includes containment zone residence while **omitting close contact with a confirmed case** (criterion 2). - Close contact was the **most common and direct mode of transmission**, making it a fundamental exposure criterion that cannot be excluded. - The distinction between area-based risk (containment zone) and person-to-person exposure (close contact) was operationally important for triage and testing priorities. *2, 3 and 4* - This option omits **travel to an affected country**, which was crucial especially in the **early pandemic phases** when imported cases were a primary concern. - Travel history was an essential screening criterion for all individuals, including pregnant women, requiring mandatory testing and quarantine. - Again, this incorrectly elevates containment zone residence to a direct exposure criterion equivalent to documented close contact or occupational exposure.
Question 2: Steroidal contraceptives available in the basket of contraceptive choice from Ministry of Health & Family Welfare, Government of India are
- A. Biphasic
- B. Estrogen only pills
- C. Monophasic (Correct Answer)
- D. Triphasic
Explanation: ***Monophasic*** - **Monophasic oral contraceptive pills** are the formulation type available in India's National Family Planning Programme basket of contraceptive choices. - The Ministry of Health & Family Welfare provides **Mala-N** (Levonorgestrel 0.15mg + Ethinyl estradiol 0.03mg) and **Mala-D** (Desogestrel + Ethinyl estradiol) - both are monophasic formulations. - Monophasic pills contain a **fixed dose of estrogen and progestin** throughout the 21 active pill cycle, making them simpler to use and ensuring better compliance. *Biphasic* - **Biphasic pills** contain two different doses of hormones during the active pill cycle. - These are **not included** in the Government of India's national family planning programme basket of contraceptive choices. - Less commonly used compared to monophasic formulations. *Estrogen only pills* - **Estrogen-only pills** are not used as contraceptives due to the risk of **endometrial hyperplasia** and cancer if not balanced with progestin. - These are used for hormone replacement therapy or specific medical conditions, **not for contraception**. *Triphasic* - **Triphasic pills** contain three different dosages of hormones throughout the active pill cycle to mimic the natural menstrual cycle. - These are **not included** in the Government of India's national family planning programme basket. - Their varied dosing schedule is more complex and not preferred for widespread public health distribution.
Question 3: The life expectancy at birth for a country A is 64 years. The minimum and maximum values of life expectancy are 20 years and 86 years respectively. As part of Human Development Index (HDI), what is the Life Expectancy Index for the country A ?
- A. 0.667 (Correct Answer)
- B. 0.512
- C. 0.970
- D. 0.744
Explanation: **0.667** - The Life Expectancy Index (LEI) is a component of the Human Development Index (HDI). - Formula: **LEI = (Actual Life Expectancy - Minimum Life Expectancy) / (Maximum Life Expectancy - Minimum Life Expectancy)** - Calculation: (64 - 20) / (86 - 20) = 44 / 66 = **0.667** - The index ranges from 0 to 1, where higher values indicate better life expectancy relative to the reference range. *0.512* - This value would result from calculation errors, such as using incorrect minimum or maximum values. - For example, if a different denominator was used or if the actual life expectancy was miscalculated. *0.970* - This value is too high and suggests a calculation error. - An index of 0.970 would indicate the country's life expectancy is 84 years (very close to the maximum of 86 years). *0.744* - This value does not correspond to the given parameters. - Could result from arithmetic errors or using different reference values for minimum/maximum life expectancy. - Using the correct formula with given values yields 0.667, not 0.744.
Question 4: Which of the following indicators stand consolidated in Physical Quality of Life Index (PQLI)? 1. Infant mortality 2. Life expectancy at age one 3. Per capita income 4. Literacy
- A. 1, 2 and 4 (Correct Answer)
- B. 1, 2 and 3
- C. 2, 3 and 4
- D. 1, 3 and 4
Explanation: ***1, 2 and 4*** - The **Physical Quality of Life Index (PQLI)** is a composite index that measures the quality of life based on three specific indicators: infant mortality, life expectancy at age one, and literacy. - These indicators were chosen to reflect basic human needs and achievements independent of economic production. *1, 2 and 3* - This option incorrectly includes **per capita income** as an indicator. The PQLI was developed as an alternative to economic measures like GDP or per capita income. - **Per capita income** is an economic indicator, whereas PQLI focuses on social indicators of well-being. *2, 3 and 4* - This option incorrectly includes **per capita income** and excludes **infant mortality**, which is a core component of the PQLI reflecting the health status of a population. - The PQLI specifically aims to capture non-economic aspects of development. *1, 3 and 4* - This option incorrectly includes **per capita income** and excludes **life expectancy at age one**, which is a critical health indicator in the PQLI. - PQLI specifically includes **life expectancy at age one** instead of other age groups to reflect achievements in reducing early childhood mortality and improving health.
Question 5: Consider the following staff: 1. Medical Officer 2. Pharmacist 3. Anaesthetist 4. Health Educator Of them, who are routinely posted to a PHC ?
- A. 1, 2 and 4 (Correct Answer)
- B. 2, 3 and 4
- C. 1, 2 and 3
- D. 1, 3 and 4
Explanation: ***1, 2 and 4*** - According to **IPHS (Indian Public Health Standards)** for PHC staffing, a **Medical Officer** is the essential physician providing primary medical care, and a **Pharmacist** is mandatory for dispensing medications and managing the drug store. - While a designated "Health Educator" post may not be uniformly established at all PHCs, **health education activities** are a core PHC function, often performed by staff nurses, ANMs, or health workers as part of their routine duties under the supervision of the Medical Officer. - In the context of this question and official guidelines, these three roles represent the personnel involved in **medical care, pharmaceutical services, and health education functions** at PHC level. *2, 3 and 4* - An **Anaesthetist** is NOT routinely posted at PHC level as PHCs do not perform surgical procedures requiring anaesthesia. - Anaesthetists are stationed at **CHCs (Community Health Centres)** with operation theatre facilities or higher-level hospitals. - This option incorrectly includes anaesthetist while omitting the essential Medical Officer. *1, 2 and 3* - While **Medical Officer** and **Pharmacist** are definitely routine PHC staff, an **Anaesthetist** is not posted at PHC level. - PHCs provide basic primary healthcare services, not surgical interventions requiring anaesthesia services. - Anaesthetists are found at CHC level and above. *1, 3 and 4* - This option incorrectly includes an **Anaesthetist** who is not a PHC-level staff member. - Additionally, it omits the **Pharmacist**, who is a mandatory and essential staff member at every PHC for medication dispensing and drug store management. - Without a pharmacist, the PHC cannot function effectively in providing essential medicines.
Question 6: Which one of the following management techniques helps in standardising the methods of performing jobs ?
- A. Work Sampling
- B. Personnel Management
- C. Systems Analysis (Correct Answer)
- D. Decision Making
Explanation: ***Systems Analysis*** - **Systems analysis** is a management technique that systematically examines processes, workflows, and organizational systems to identify inefficiencies and standardize operations. - It helps in **standardizing methods of performing jobs** by breaking down complex tasks into components, analyzing each step, and establishing uniform procedures and protocols. - In public health administration, systems analysis is used to create **standard operating procedures (SOPs)** and ensure consistency in service delivery. - This is the **best answer** among the given options for standardizing job methods. *Work Sampling* - **Work sampling** is a work measurement technique that uses random observations to determine the proportion of time workers spend on various activities. - Its primary purpose is **data collection and time measurement**, not the standardization of how tasks should be performed. - It helps identify *what* workers do, but not *how* to standardize the methods. *Personnel Management* - **Personnel management** deals with human resource functions including recruitment, training, performance appraisal, and employee welfare. - While training may involve teaching standardized methods, personnel management itself is **not a technique for standardizing job methods**. - It focuses on managing people, not on analyzing and standardizing work processes. *Decision Making* - **Decision making** is a cognitive and managerial process of choosing between alternatives to achieve organizational goals. - It is a **general management function**, not a specific technique for analyzing and standardizing how jobs are performed. - While decisions may lead to standardization, decision making itself is not the technique that accomplishes it.
Question 7: STDs are transmitted by
- A. Contact with soil
- B. Droplet infection
- C. Vector borne
- D. Direct contact (Correct Answer)
Explanation: ***Direct contact*** - **Sexually Transmitted Diseases (STDs)** are primarily spread through direct physical contact, most commonly during **sexual activity** (vaginal, anal, or oral sex). - This mode of transmission allows for the exchange of infected bodily fluids or skin-to-skin contact, leading to the spread of pathogens like bacteria, viruses, or parasites. *Contact with soil* - Diseases transmitted through contact with soil, such as **tetanus** or **hookworm infections**, typically involve pathogens that reside in the soil. - This is not a primary mode of transmission for common STDs. *Droplet infection* - **Droplet infection** involves the transmission of pathogens through respiratory droplets expelled during coughing, sneezing, or talking, like in **influenza** or **tuberculosis**. - STDs are generally not aerosolized and do not spread through this route. *Vector borne* - **Vector-borne diseases** are transmitted by an intermediate organism, often an insect (e.g., **mosquitoes** for malaria, **ticks** for Lyme disease). - STDs do not rely on vectors for transmission between human hosts.
Question 8: In which one of the following study designs, the unit of study involves populations rather than individuals ?
- A. Cross-sectional studies
- B. Cohort studies
- C. Ecological studies (Correct Answer)
- D. Case-control studies
Explanation: ***Correct: Ecological studies*** - **Ecological studies** analyze health-related data at a population level, such as countries or communities, rather than individual patients. - They are used to observe correlations between exposure and outcome among different groups or over time. - The unit of analysis is the **population or group**, not individuals. *Incorrect: Cross-sectional studies* - **Cross-sectional studies** examine individuals at a single point in time to determine the prevalence of a disease or exposure. - While they can describe populations, the unit of observation and analysis remains the **individual**. *Incorrect: Cohort studies* - **Cohort studies** follow groups of individuals (cohorts) over time to investigate the incidence of an outcome and its association with specific exposures. - The primary unit of study is the **individual**, who is tracked for disease development. *Incorrect: Case-control studies* - **Case-control studies** compare individuals with a disease (cases) to individuals without the disease (controls) to identify past exposures. - This design focuses on **individual-level data** to determine risk factors.
Question 9: What is the Standardized Mortality Ratio (SMR) for the hazardous industry workers (as compared to national population)?
- A. 110
- B. 100
- C. 120 (Correct Answer)
- D. 130
Explanation: ***120*** - To calculate the Standardized Mortality Ratio (SMR), we first need to calculate the **expected deaths** for the hazardous industry workers based on the national death rates. - The formula for expected deaths in each age group is: (National death rate / 1000) × Number of hazardous industry workers - For age group 25-34: Expected deaths = (2.0 / 1000) × 3000 = **6** - For age group 35-44: Expected deaths = (3.5 / 1000) × 2000 = **7** - For age group 45-54: Expected deaths = (6.0 / 1000) × 2000 = **12** - **Total expected deaths** = 6 + 7 + 12 = **25** - **Total observed deaths** = 8 + 9 + 13 = **30** - **SMR formula**: (Total Observed Deaths / Total Expected Deaths) × 100 - **SMR = (30 / 25) × 100 = 1.2 × 100 = 120** - This indicates that the hazardous industry workers have a **20% higher mortality rate** compared to the national population after age-standardization. *100* - An SMR of 100 would indicate that the observed mortality equals the expected mortality (no difference from the national average). - However, the observed deaths (30) exceed the expected deaths (25), so the SMR must be greater than 100. - This option represents the null value where there is no excess mortality. *110* - This option underestimates the actual SMR calculated from the data. - An SMR of 110 would suggest only a 10% excess mortality, which does not match the observed-to-expected ratio of 30:25. - The calculation clearly shows a ratio of 1.2, not 1.1. *130* - This option overestimates the SMR. - An SMR of 130 would require observed deaths to be 1.3 times the expected deaths (32.5 deaths expected for 30 observed). - The actual ratio is 30/25 = 1.2, making this value too high.
Question 10: Which one of the following best explains the relationship among Prevalence (P), Incidence (I) and Duration (D) of a disease given the assumption that the population is stable ?
- A. I = P x D
- B. P = I x D (Correct Answer)
- C. D = P x I
- D. I = P + D
Explanation: **Fundamental Epidemiological Relationship:** In a stable population with endemic disease, the relationship between prevalence, incidence, and duration is expressed as: **Prevalence = Incidence × Average Duration (P = I × D)** ***P = I × D*** - This is the **correct formula** that describes the relationship under conditions of a **stable population** and **endemic disease**. - Prevalence is directly proportional to both the incidence rate and the average duration of the disease. - This formula reflects that the number of existing cases (prevalence) equals the rate at which new cases occur (incidence) multiplied by how long people have the disease (duration). - Example: If incidence = 10 cases/1000/year and average duration = 5 years, then prevalence = 50 cases/1000. *I = P × D* - This formula incorrectly suggests that incidence increases with both prevalence and duration. - This would mean that longer disease duration causes higher incidence, which is illogical. - Correctly rearranged, this would be I = P/D (incidence equals prevalence divided by duration). *D = P × I* - This formula incorrectly states that duration is the product of prevalence and incidence. - This would mean higher incidence causes longer duration, which is epidemiologically incorrect. - Correctly rearranged, this would be D = P/I (duration equals prevalence divided by incidence). *I = P + D* - This formula implies a simple additive relationship, which is **epidemiologically invalid**. - Prevalence, incidence, and duration are related **multiplicatively**, not additively, in a steady state. - This equation has no basis in epidemiological theory.