All (378)Anatomy (22)Anatomy (5)Anesthesiology (9)Behavioral Science (1)Biochemistry (3)Biochemistry (21)Biostatistics (4)Community Medicine (20)Dermatology (13)Diagnosis (3)ENT (11)Forensic Medicine (13)General Medicine (1)Internal Medicine (19)Internal Medicine (26)Microbiology (20)OB/GYN (16)Obstetrics and Gynecology (16)Ophthalmology (10)Orthopaedics (14)Pathology (25)Pediatrics (18)Pediatrics (2)Pharmacology (37)Physiology (10)Psychiatry (6)Radiology (12)Surgery (21)
Q51
A patient underwent a gastrectomy. Which vitamin replacement is required?
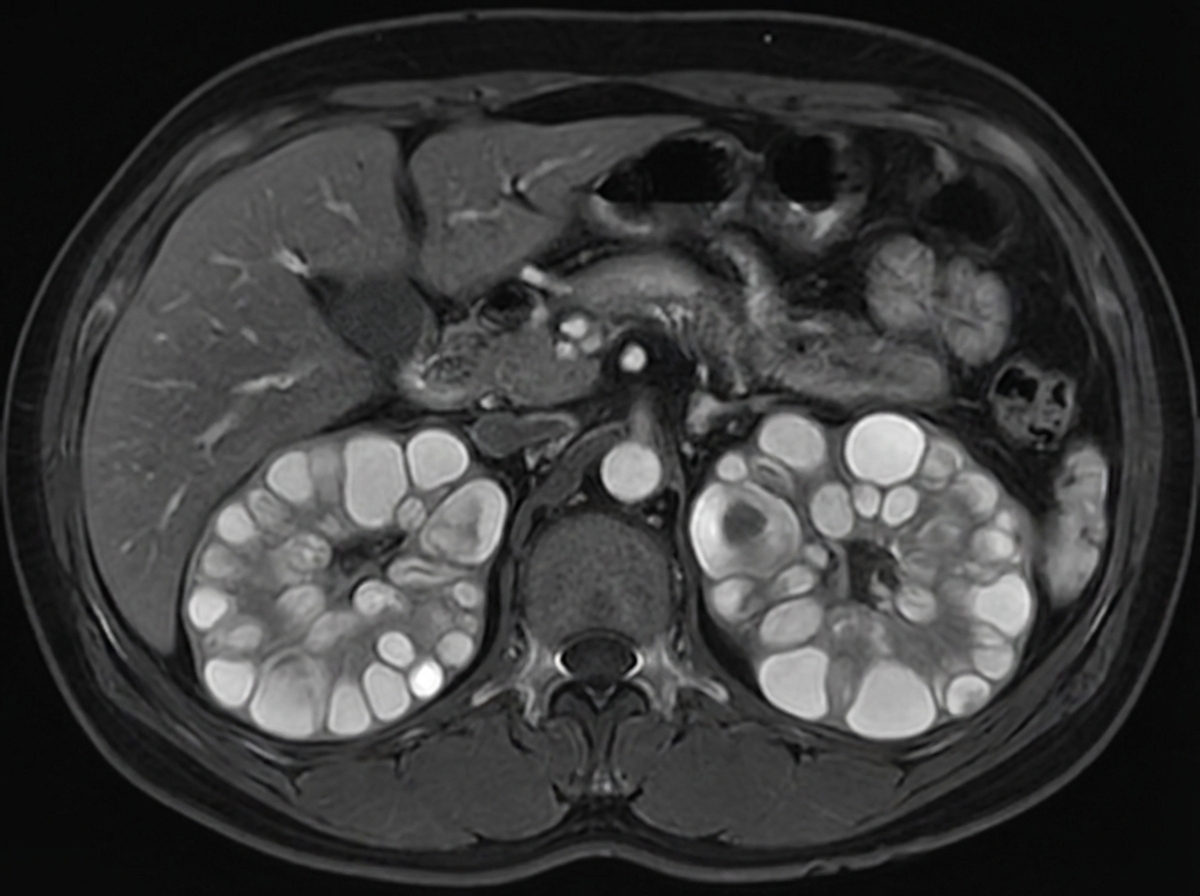
Q52
A 45-year-old patient presents with hypertension, hematuria, and flank pain. An MRI scan is performed, and the image provided shows multiple cystic lesions in both kidneys. What is the most likely diagnosis?
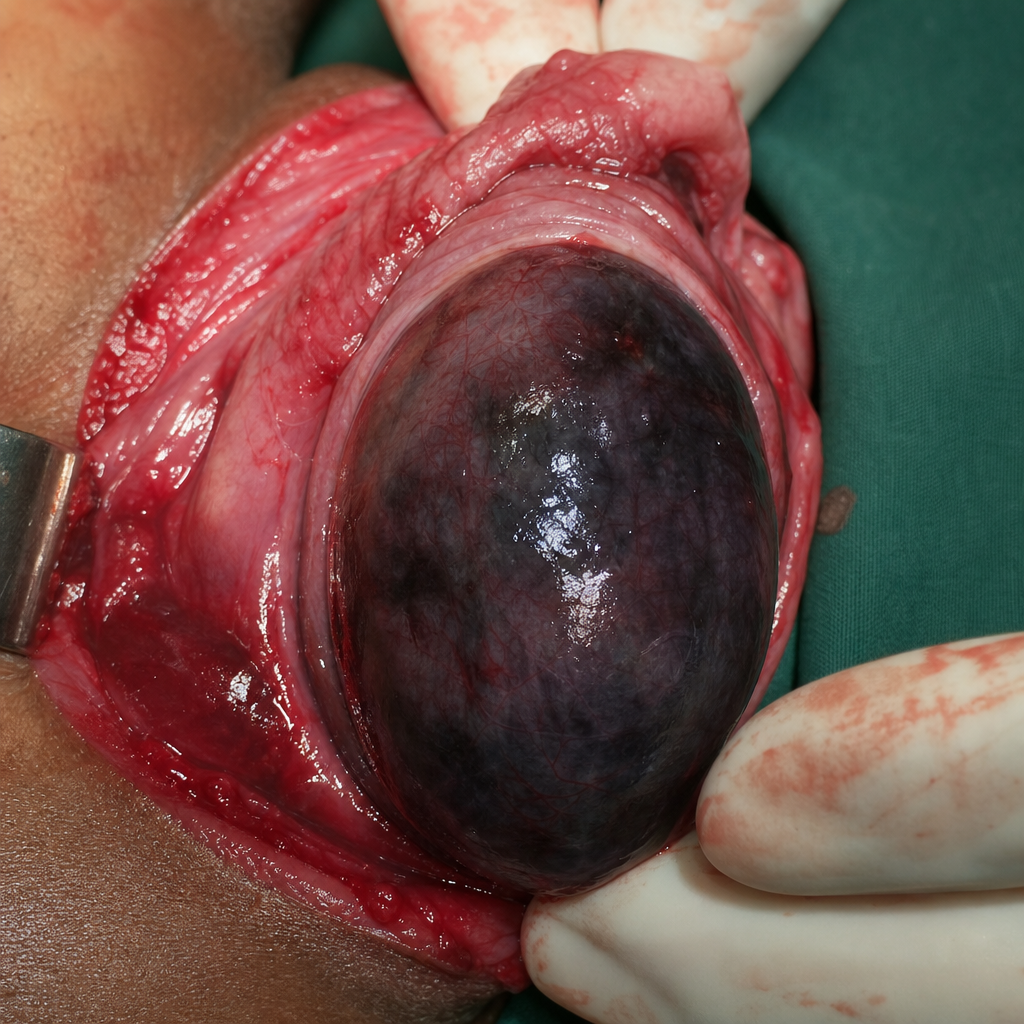
Q53
An endoscopic image shows the following finding. What is the most likely diagnosis?