NEET-PG 2023 — Pharmacology
15 Previous Year Questions with Answers & Explanations
Claviceps purpurea produces which of the following toxins?
A patient on atracurium develops seizures due to accumulation of which substance?
A child presented with a history of ingestion of an unknown plant and developed mydriasis, tachycardia, dry mouth, warm skin, and delirium. Which of the following groups of drugs is likely to be responsible for the symptoms of this child?
Which of the following drugs inhibits the activation of plasminogen?
Which of the following clotting factors in a patient on Warfarin therapy would show the earliest decrease in functional activity?
A patient with a malignancy is undergoing chemotherapy. The platelet counts were reduced after the previous cycle of chemotherapy. Which of the following drugs can be used to treat this patient?
A patient who is a known case of hypertension on multiple anti-hypertensive medications came to OPD. His ECG finding is given below. Which of the following drugs is responsible for the ECG finding? (Image of ECG finding)
A 3-week-old infant presents with a cough and sore throat. The mother reports that the infant develops a paroxysm of cough followed by apnea. The total leucocyte count is >50,000 cells/μL. Based on these symptoms, which of the following drugs is the most appropriate treatment for this patient?
A patient with recurrent gout attacks was started on a drug that inhibits uric acid synthesis. His symptoms were reduced after therapy. Which drug was he started on?
A patient given digoxin started having side effects like nausea and vomiting. The serum concentration of digoxin was 4 ng/mL. The plasma therapeutic range is 1-2 ng/mL. If the half-life of digoxin is 40 hours, how long should one wait before resuming the treatment?
NEET-PG 2023 - Pharmacology NEET-PG Practice Questions and MCQs
Question 1: Claviceps purpurea produces which of the following toxins?
- A. Ergot alkaloids (Correct Answer)
- B. Aflatoxins
- C. Sanguinarine alkaloid
- D. Pyrazolidone drug
Explanation: ***Ergot alkaloids*** - **Claviceps purpurea** is a fungus that infects cereals, particularly rye, and produces a group of toxic compounds known as **ergot alkaloids**. - These alkaloids can cause a condition called **ergotism**, which includes symptoms like hallucinations, gangrene, and severe vasoconstriction. *Aflatoxins* - **Aflatoxins** are produced by species of **Aspergillus fungi**, such as *A. flavus* and *A. parasiticus*, not *Claviceps purpurea*. - They are potent **carcinogens** and are commonly found in contaminated crops like peanuts and maize. *Sanguinarine alkaloid* - **Sanguinarine** is an alkaloid derived from plants like **bloodroot (Sanguinaria canadensis)**, not *Claviceps purpurea*. - It has been linked to **glaucoma** and liver toxicity. *Pyrazolidone drug* - **Pyrazolidone** is a classification of synthetic drugs, often used as **non-steroidal anti-inflammatory drugs (NSAIDs)**, such as phenylbutazone. - This is a pharmaceutical compound and not naturally derived from *Claviceps purpurea* or any fungus.
Question 2: A patient on atracurium develops seizures due to accumulation of which substance?
- A. Atracurium acid
- B. Laudanosine (Correct Answer)
- C. Cisatracurium
- D. Histamine
Explanation: ***Laudanosine*** - Atracurium is metabolized into **laudanosine**, a **neurotoxic metabolite** that can accumulate, particularly in patients with renal or hepatic dysfunction, leading to **seizures** and central nervous system excitation. - Due to its potential for neurotoxicity, atracurium is often replaced by **cisatracurium**, which produces less laudanosine. *Cisatracurium* - **Cisatracurium** is an isomer of atracurium that is also metabolized via **Hofmann elimination** but produces significantly **less laudanosine**. - It is preferred in patients with **renal or hepatic impairment** due to its reduced potential for metabolite accumulation and neurotoxicity. *Atracurium acid* - Atracurium acid is one of the **inactive metabolites** of atracurium, along with laudanosine. - Unlike laudanosine, atracurium acid is **not neurotoxic** and does not contribute to seizure activity. *Histamine* - Atracurium can cause an **immediate release of histamine**, leading to transient hypotension, flushing, and bronchospasm, especially with rapid bolus injection. - While histamine release is an adverse effect of atracurium, it is **not directly responsible for seizure activity**.
Question 3: A child presented with a history of ingestion of an unknown plant and developed mydriasis, tachycardia, dry mouth, warm skin, and delirium. Which of the following groups of drugs is likely to be responsible for the symptoms of this child?
- A. Anticholinergic (Correct Answer)
- B. Sympathomimetic
- C. Opioid
- D. Benzodiazepine
Explanation: ***Anticholinergic*** - The constellation of mydriasis, tachycardia, dry mouth, warm skin, and delirium is classic for **anticholinergic toxicity**, often described as "hot as a hare, blind as a bat, dry as a bone, red as a beet, and mad as a hatter." - This toxidrome is caused by the blockade of **muscarinic acetylcholine receptors**, leading to widespread inhibition of parasympathetic nervous system functions. - Common plant sources include **Datura** (jimsonweed) and **Atropa belladonna** (deadly nightshade). *Sympathomimetic* - While **mydriasis** and **tachycardia** can be present, sympathomimetic toxicity typically causes **diaphoresis (sweating)** and **hypertension**, not dry skin and mouth. - Patients often present with agitation, paranoia, and potentially seizures, but the key differentiating factor is the presence of profuse sweating. *Opioid* - Opioid overdose is characterized by the classic triad of **miosis (pinpoint pupils)**, **respiratory depression**, and **CNS depression (coma)**, none of which are present in this case. - Other common symptoms include bradycardia, hypotension, and hypothermia, which are contrary to the child's presentation. *Benzodiazepine* - Benzodiazepine overdose typically causes **CNS depression** including drowsiness, ataxia, and slurred speech, but usually spares vital signs unless combined with other depressants. - **Mydriasis**, **tachycardia**, and **dry mouth** are not characteristic symptoms of benzodiazepine toxicity; pupils are typically normal or slightly dilated due to hypoxia in severe cases.
Question 4: Which of the following drugs inhibits the activation of plasminogen?
- A. Streptokinase
- B. Aminocaproic acid (Correct Answer)
- C. Reteplase
- D. Clopidogrel
Explanation: ***Correct Option: Aminocaproic acid*** - **Aminocaproic acid** is an antifibrinolytic drug that acts by competitively inhibiting the activation of **plasminogen** to plasmin. - By preventing the formation of plasmin, it stabilizes blood clots and is used to treat excessive bleeding. *Incorrect Option: Streptokinase* - **Streptokinase** is a **thrombolytic agent** that forms a complex with plasminogen, converting uncomplexed plasminogen into plasmin. - This action promotes the degradation of fibrin clots, making it a **fibrinolytic drug**, not an inhibitor of plasminogen activation. *Incorrect Option: Reteplase* - **Reteplase** is a **recombinant tissue plasminogen activator (tPA)** that directly converts plasminogen to plasmin. - This drug actively promotes **fibrinolysis** and clot breakdown, making it a thrombolytic agent. *Incorrect Option: Clopidogrel* - **Clopidogrel** is an **antiplatelet drug** that inhibits platelet aggregation by irreversibly blocking the P2Y12 adenosine diphosphate (ADP) receptor on platelets. - Its mechanism of action is focused on **platelet function**, not on the plasminogen-plasmin system.
Question 5: Which of the following clotting factors in a patient on Warfarin therapy would show the earliest decrease in functional activity?
- A. Factor VII (Correct Answer)
- B. Factor IX
- C. Factor X
- D. Prothrombin (Factor 2)
Explanation: ***Factor VII*** - Factor VII has the **shortest half-life** (approximately 6 hours) among the vitamin K-dependent clotting factors, meaning its functional activity decreases **most rapidly** after starting warfarin therapy. - Warfarin inhibits vitamin K epoxide reductase, preventing gamma-carboxylation of **all vitamin K-dependent factors** (II, VII, IX, X). However, Factor VII's short half-life means pre-existing functional Factor VII is depleted first. - This is why **PT/INR** (which measures the extrinsic pathway dependent on Factor VII) rises before aPTT in warfarin therapy. - Reduced gamma-carboxylation impairs Factor VII's ability to bind calcium and phospholipids, essential for its activation in the extrinsic coagulation pathway. *Factor IX* - Factor IX is a **vitamin K-dependent factor** affected by warfarin, but its longer half-life (approximately 24 hours) means functional activity decreases more slowly than Factor VII. - It plays a key role in the **intrinsic coagulation pathway**. *Factor X* - Factor X is a **vitamin K-dependent clotting factor** whose gamma-carboxylation is inhibited by warfarin. - Its half-life (approximately 40 hours) is longer than Factor VII, resulting in a **slower decline in functional activity**. *Prothrombin (Factor II)* - Prothrombin (Factor II) is a **vitamin K-dependent factor** affected by warfarin. - It has the **longest half-life** (60-72 hours) among vitamin K-dependent factors, meaning its functional levels decrease most slowly after initiating warfarin therapy.
Question 6: A patient with a malignancy is undergoing chemotherapy. The platelet counts were reduced after the previous cycle of chemotherapy. Which of the following drugs can be used to treat this patient?
- A. Oprelvekin (IL-11) - stimulates platelet production (Correct Answer)
- B. Filgrastim - stimulates white blood cell production
- C. Amifostine - protects against chemotherapy toxicity
- D. Erythropoietin - stimulates red blood cell production
Explanation: ***Oprelvekin (IL-11) - stimulates platelet production*** - **Oprelvekin** is a recombinant interleukin-11 (IL-11) that directly stimulates the proliferation and maturation of **megakaryocytes**, leading to increased platelet production. - It is specifically indicated for the prevention of **severe thrombocytopenia** and the reduction of the need for platelet transfusions following myelosuppressive chemotherapy. *Filgrastim - stimulates white blood cell production* - **Filgrastim** is a **granulocyte colony-stimulating factor (G-CSF)** that primarily acts on neutrophil precursors, promoting their proliferation and maturation. - It is used to prevent and treat **neutropenia** and reduce the incidence of febrile neutropenia, but it does not significantly affect platelet counts. *Amifostine - protects against chemotherapy toxicity* - **Amifostine** is a **cytoprotective agent** that reduces toxicities associated with chemotherapy and radiation by preferentially protecting non-malignant cells. - It does not directly stimulate blood cell production but rather acts as a **free radical scavenger** to mitigate damage from cytotoxic treatments. *Erythropoietin - stimulates red blood cell production* - **Erythropoietin** is a **hematopoietic growth factor** that specifically stimulates the production of **red blood cells** by promoting the proliferation and differentiation of erythroid progenitor cells. - It is used to treat **anemia**, particularly in patients with chronic kidney disease or those undergoing chemotherapy, but it has no role in managing thrombocytopenia.
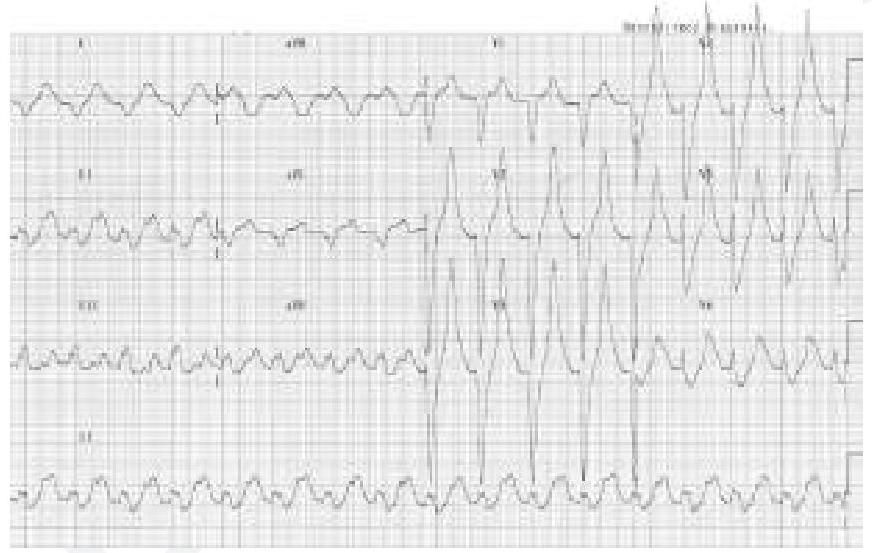
Question 7: A patient who is a known case of hypertension on multiple anti-hypertensive medications came to OPD. His ECG finding is given below. Which of the following drugs is responsible for the ECG finding? (Image of ECG finding)
- A. Prazosin
- B. Metoprolol
- C. Hydrochlorothiazide
- D. Spironolactone (Correct Answer)
Explanation: ***Spironolactone*** - The ECG shows a **tall, peaked T wave**, which is characteristic of **hyperkalemia**. - **Spironolactone** is a **potassium-sparing diuretic**, and its use, especially in combination with other medications or in patients with **renal impairment**, can lead to **hyperkalemia**. *Prazosin* - Prazosin is an **alpha-1 adrenergic blocker** used for **hypertension**. - It does **not directly affect potassium levels** and is not associated with the ECG changes seen in hyperkalemia. *Metoprolol* - Metoprolol is a **beta-blocker** primarily used for **hypertension**, **angina**, and **arrhythmias**. - It does **not significantly cause hyperkalemia** or the characteristic ECG changes shown. *Hydrochlorothiazide* - Hydrochlorothiazide is a **thiazide diuretic** that typically causes **hypokalemia**, not hyperkalemia, by **increasing potassium excretion**. - The ECG findings associated with hypokalemia would include **flattened T waves** or **prominent U waves**.
Question 8: A 3-week-old infant presents with a cough and sore throat. The mother reports that the infant develops a paroxysm of cough followed by apnea. The total leucocyte count is >50,000 cells/μL. Based on these symptoms, which of the following drugs is the most appropriate treatment for this patient?
- A. Azithromycin (Correct Answer)
- B. Amoxicillin
- C. Cotrimoxazole
- D. Erythromycin
Explanation: ***Azithromycin*** - This infant's symptoms are highly suggestive of **pertussis** (whooping cough), characterized by **paroxysmal coughs** followed by **apnea** in young infants, along with **marked leukocytosis**. - **Macrolides** are the treatment of choice due to their effectiveness against *Bordetella pertussis*; **azithromycin** is preferred in infants due to better tolerability and a shorter course compared to erythromycin. *Amoxicillin* - **Amoxicillin** is a penicillin-class antibiotic primarily effective against various bacterial respiratory infections, but it has **no activity against *Bordetella pertussis***. - Using amoxicillin for pertussis would lead to **treatment failure** and a worsening of the infant's condition. *Cotrimoxazole* - While **cotrimoxazole** (trimethoprim-sulfamethoxazole) can be used as an alternative for pertussis in patients **allergic to macrolides**, it is **not the first-line treatment** in infants. - It carries a risk of **kernicterus** in newborns and young infants due to displacement of bilirubin from albumin, so it is generally avoided. *Erythromycin* - **Erythromycin** is a macrolide and is effective against *Bordetella pertussis*, but it is **associated with a higher incidence of infantile hypertrophic pyloric stenosis** when given to young infants. - Due to this adverse effect, **azithromycin** is generally preferred over erythromycin in infants for pertussis treatment.
Question 9: A patient with recurrent gout attacks was started on a drug that inhibits uric acid synthesis. His symptoms were reduced after therapy. Which drug was he started on?
- A. Probenecid
- B. Colchicine
- C. Diclofenac
- D. Allopurinol (Correct Answer)
Explanation: ***Allopurinol*** - **Allopurinol** is a **xanthine oxidase inhibitor** that effectively reduces uric acid synthesis by blocking the enzyme responsible for converting hypoxanthine and xanthine to uric acid. - It is a cornerstone therapy for preventing recurrent gout attacks in patients with **hyperuricemia**. *Probenecid* - **Probenecid** is a **uricosuric agent** that increases the excretion of uric acid in the urine, rather than inhibiting its synthesis. - It works by inhibiting the reabsorption of uric acid in the renal tubules. *Colchicine* - **Colchicine** is an **anti-inflammatory agent** primarily used to treat acute gout flares and prevent future attacks by disrupting microtubule function and inhibiting neutrophil migration. - It does not affect uric acid synthesis or excretion. *Diclofenac* - **Diclofenac** is a **non-steroidal anti-inflammatory drug (NSAID)** used to manage the pain and inflammation associated with acute gout attacks. - It works by inhibiting prostaglandin synthesis and has no effect on uric acid levels.
Question 10: A patient given digoxin started having side effects like nausea and vomiting. The serum concentration of digoxin was 4 ng/mL. The plasma therapeutic range is 1-2 ng/mL. If the half-life of digoxin is 40 hours, how long should one wait before resuming the treatment?
- A. 120 hours
- B. 140-180 hours
- C. 1 half-life (40 hours)
- D. 80 hours (Correct Answer)
Explanation: ***80 hours (2 half-lives)***- Current digoxin level is **4 ng/mL**, which is **twice the upper therapeutic limit** (2 ng/mL), causing toxicity with nausea and vomiting [1]- After **1 half-life (40 hours)**: concentration reduces to 2 ng/mL (upper therapeutic limit) [2]- After **2 half-lives (80 hours)**: concentration reduces to 1 ng/mL (mid-therapeutic range) [2]- **Clinical rationale**: While 2 ng/mL is technically within range, waiting for 2 half-lives ensures the level is comfortably in the **middle of the therapeutic window** (1 ng/mL), providing a **safer margin** before resuming treatment in a patient who just experienced toxicity- This conservative approach minimizes risk of recurrent toxicity, especially important given the patient's recent symptoms at 4 ng/mL*1 half-life (40 hours)*- After 1 half-life, digoxin level would be 2 ng/mL, which is at the **upper limit** of the therapeutic range- While technically within the therapeutic range, this leaves **minimal safety margin** in a patient who just experienced toxicity- Starting treatment immediately at this level carries higher risk of recurrent side effects*120 hours (3 half-lives)*- After 3 half-lives, the concentration would be **0.5 ng/mL**, which is **below the therapeutic range** (1-2 ng/mL)- This is overly conservative and would **unnecessarily delay** resumption of essential cardiac medication- Could lead to inadequate control of the underlying condition (heart failure or atrial fibrillation)*140-180 hours (3.5-4.5 half-lives)*- This would reduce digoxin to **0.25-0.35 ng/mL**, well below therapeutic levels- This **excessive delay** is not clinically justified and could worsen the patient's cardiac condition- No standard protocol recommends waiting this long before resuming digoxin therapy