NEET-PG 2023 — Pediatrics
11 Previous Year Questions with Answers & Explanations
A 4-year-old child is brought to the emergency department with severe dehydration due to diarrhea. What is the initial management for severe dehydration?
What is the most common cause of conjugated hyperbilirubinemia in infants?
A child was brought with pedal edema and cheilosis. Cardiomegaly was present. What is the vitamin deficiency associated with this clinical presentation?
An infant presents with hepatosplenomegaly and thrombocytopenia. Neuroimaging with CT shows periventricular calcifications. What is the most likely diagnosis?
Which of the following is the best sign to indicate adequate growth in an infant with a birth weight of 2.8 kg?
A 3-month-old baby presents with deafness, cataract, and patent ductus arteriosus. Which of the following is the most likely diagnosis?
A child presents with a fever and a rash. Urine examination showed cells with owl's eye appearance. What is the most likely diagnosis?
Which vitamin deficiency is most commonly associated with rickets in children?
A 2-year-old child with a history of eczema presents with a red, scaly rash around the mouth and extremities. A dietary history reveals excessive consumption of cow's milk. What nutritional deficiency is most likely?
A 2 year child presented with low grade fever and stridor. What is the likely diagnosis?
NEET-PG 2023 - Pediatrics NEET-PG Practice Questions and MCQs
Question 1: A 4-year-old child is brought to the emergency department with severe dehydration due to diarrhea. What is the initial management for severe dehydration?
- A. Oral rehydration therapy
- B. Intravenous fluids (Correct Answer)
- C. Antidiarrheal medication
- D. Antibiotics
Explanation: ***Intravenous fluids*** - For **severe dehydration**, rapid correction of fluid and electrolyte imbalances is critical, and **intravenous fluids** (normal saline or Ringer's lactate) are the **first-line treatment**. - As per **WHO and IAP guidelines**, children with severe dehydration require **IV fluid resuscitation** at 100 mL/kg over 3-6 hours (or 30 mL/kg bolus initially). - Signs of severe dehydration include **lethargy, sunken eyes, absent tears, very dry mucous membranes, poor skin turgor**, and inability to drink. - IV route ensures **rapid intravascular volume expansion** when oral intake is compromised or inadequate. *Oral rehydration therapy* - **ORT** is the treatment of choice for **mild to moderate dehydration only** (Plan B as per WHO). - In severe dehydration, children often have **altered consciousness, persistent vomiting**, or **circulatory compromise**, making oral intake ineffective or impossible. - ORT can be initiated once the child is alert and able to drink after initial IV resuscitation. *Antidiarrheal medication* - **Not recommended** in children with acute diarrhea, especially under 5 years. - Medications like loperamide can cause **ileus, drowsiness**, and may worsen outcomes. - They do **not address fluid and electrolyte deficits**, which is the immediate life-threatening concern. *Antibiotics* - Only indicated for **specific bacterial causes** (e.g., cholera, shigellosis with blood in stool, or proven invasive bacterial infection). - **Not part of initial management** for severe dehydration. - Indiscriminate use contributes to **antibiotic resistance** and delays critical rehydration.
Question 2: What is the most common cause of conjugated hyperbilirubinemia in infants?
- A. Rotor syndrome
- B. Crigler Najjar syndrome
- C. Dubin-Johnson syndrome
- D. Biliary atresia (Correct Answer)
Explanation: ***Rotor syndrome*** - Characterized by **conjugated hyperbilirubinemia** due to a defect in hepatic uptake and storage of bilirubin [1]. - This condition can lead to elevated levels of **direct (conjugated) bilirubin** without significant liver damage. *Crigler Najjar* - This condition primarily causes **unconjugated hyperbilirubinemia** due to a deficiency of the enzyme **uridine diphosphate glucuronyl transferase** [1]. - It typically presents with **kernicterus** in newborns rather than conjugated bilirubin elevation. *Breast milk jaundice* - Mainly leads to **unconjugated hyperbilirubinemia** due to substances in breast milk that inhibit bilirubin conjugation. - Generally occurs in **breastfed infants** after the first week of life, not presenting with increased conjugated bilirubin. *Gilbert syndrome* - This syndrome is associated with **unconjugated hyperbilirubinemia** due to a genetic defect in bilirubin conjugation [1]. - Typically benign, it does not cause **increased conjugated bilirubin** levels as seen in Rotor syndrome. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Liver and Gallbladder, p. 860.
Question 3: A child was brought with pedal edema and cheilosis. Cardiomegaly was present. What is the vitamin deficiency associated with this clinical presentation?
- A. Riboflavin deficiency
- B. Thiamine deficiency (Correct Answer)
- C. Pyridoxine deficiency
- D. Niacin deficiency
Explanation: ***Thiamine deficiency*** - The combination of **pedal edema** and **cardiomegaly** suggests **wet beriberi**, which is caused by **thiamine (vitamin B1) deficiency**. - **Cheilosis** (cracking at the corners of the mouth) is also a feature that can be seen in various vitamin deficiencies, but the cardiac involvement is highly indicative of thiamine deficiency. *Riboflavin deficiency* - **Riboflavin (vitamin B2) deficiency** is characterized by **cheilosis**, glossitis, angular stomatitis, and seborrheic dermatitis. - It typically does not cause **cardiomegaly** or significant **pedal edema** without other concurrent nutritional deficiencies. *Pyridoxine deficiency* - **Pyridoxine (vitamin B6) deficiency** primarily manifests as **dermatitis**, **microcytic anemia**, and neurological symptoms like **peripheral neuropathy** and **seizures**. - It is not typically associated with **pedal edema** or **cardiomegaly**. *Niacin deficiency* - **Niacin (vitamin B3) deficiency** causes **pellagra**, characterized by the "3 Ds": **dermatitis**, **diarrhea**, and **dementia**. - While it can manifest with systemic issues, it does not typically present with the prominent **cardiomegaly** and **pedal edema** seen in this case.
Question 4: An infant presents with hepatosplenomegaly and thrombocytopenia. Neuroimaging with CT shows periventricular calcifications. What is the most likely diagnosis?
- A. Congenital rubella syndrome
- B. Congenital herpes simplex virus infection
- C. Congenital toxoplasmosis
- D. Congenital cytomegalovirus infection (Correct Answer)
Explanation: ***Congenital cytomegalovirus infection*** - **Periventricular calcifications** on neuroimaging are a classic and highly suggestive finding for congenital CMV infection. - **Hepatosplenomegaly** and **thrombocytopenia** are common systemic manifestations of congenital CMV, which can be severe. *Congenital rubella syndrome* - Rubella typically causes **sensorineural hearing loss**, ocular abnormalities (e.g., cataracts), and congenital heart defects (e.g., patent ductus arteriosus), rather than periventricular calcifications. - While hepatosplenomegaly and thrombocytopenia can occur, the specific brain calcification pattern points away from rubella. *Congenital herpes simplex virus infection* - HSV infection in neonates presents with a variety of symptoms, including skin vesicles, keratoconjunctivitis, and seizures. - Brain imaging often shows **focal necrosis** or **encephalitis**, not typically periventricular calcifications unless it's a very widespread and destructive process. *Congenital toxoplasmosis* - Congenital toxoplasmosis classic triad includes **chorioretinitis**, **hydrocephalus**, and **intracranial calcifications**, but these calcifications are typically scattered or diffuse rather than strictly periventricular. - While hepatosplenomegaly and thrombocytopenia can be present, the specific location of calcifications is a key differentiating factor.
Question 5: Which of the following is the best sign to indicate adequate growth in an infant with a birth weight of 2.8 kg?
- A. Increase in length of 25 centimetres in the first year (Correct Answer)
- B. Weight gain of 300 grams per month till 1 year
- C. Anterior fontanelle closure by 6 months of age
- D. Weight under the 75th percentile and height under the 25th percentile
Explanation: ***Increase in length of 25 centimetres in the first year*** - A **25 cm increase in length during the first year** is a normal and expected growth rate for infants, indicating adequate overall growth and development since overall length growth is a sensitive indicator of good health. - This corresponds to roughly a **50% increase in birth length** (which is typically around 50 cm), demonstrating appropriate linear growth. *Weight gain of 300 grams per month till 1 year* - While weight gain is crucial, an infant typically **gains more than 300 grams per month** in the early months (e.g., 500-1000g/month for the first 3-4 months) and then the rate slows. - This value represents an **average over the entire year** and may not reflect adequate growth during periods of rapid weight gain. *Anterior fontanelle closure by 6 months of age* - The **anterior fontanelle typically closes between 10 to 18 months of age**, with closure as early as 6 months being within the normal range but not the *best* indicator of overall growth. - While fontanelle closure is an important developmental milestone, it is **not a direct measure of growth in length or weight**, which are more indicative of nutritional status. *Weight under the 75th percentile and height under the 25th percentile* - Having weight under the 75th percentile and height under the 25th percentile means the **child is growing disproportionately**, which could suggest a growth problem or underlying health issue. - **Optimal growth** is typically indicated when weight and height measurements fall within a similar percentile range, generally between the 25th and 75th percentiles.
Question 6: A 3-month-old baby presents with deafness, cataract, and patent ductus arteriosus. Which of the following is the most likely diagnosis?
- A. Congenital herpes simplex virus infection
- B. Congenital toxoplasmosis
- C. Congenital cytomegalovirus infection
- D. Congenital rubella syndrome (Correct Answer)
Explanation: ***Congenital rubella syndrome*** - The classic triad of **deafness**, **cataracts**, and **patent ductus arteriosus (PDA)** is highly characteristic of congenital rubella syndrome. - This syndrome results from **maternal rubella infection** during the first trimester of pregnancy. *Congenital herpes simplex virus infection* - Typically presents with **skin vesicles**, **keratoconjunctivitis**, and **encephalitis**. - **Deafness, cataracts, and PDA** are not common features of congenital HSV. *Congenital toxoplasmosis* - The classic triad involves **chorioretinitis**, **hydrocephalus**, and **intracranial calcifications**. - While it can cause microcephaly and seizures, **deafness, cataracts, and PDA** are not hallmark features. *Congenital cytomegalovirus infection* - Often causes **sensorineural hearing loss** and sometimes **chorioretinitis**, but the combination with **cataracts** and **PDA** is atypical. - Other common features include **periventricular calcifications**, **hepatosplenomegaly**, and **thrombocytopenia**.
Question 7: A child presents with a fever and a rash. Urine examination showed cells with owl's eye appearance. What is the most likely diagnosis?
- A. Herpes simplex virus infection
- B. Toxoplasmosis caused by Toxoplasma gondii
- C. Cytomegalovirus (CMV) infection (Correct Answer)
- D. Infectious mononucleosis caused by Epstein-Barr virus
Explanation: ***Cytomegalovirus (CMV) infection*** - The presence of cells with an **owl's eye appearance** in urine sediment is a classic histological hallmark of **CMV infection**. - CMV can cause a variety of symptoms in children, including **fever and rash**, making this the most likely diagnosis. *Herpes simplex virus infection* - HSV causes characteristic **vesicular lesions** on mucocutaneous surfaces, often associated with fever. - While HSV can cause systemic illness, it does not typically present with **owl's eye inclusions** in urine cells. *Toxoplasmosis caused by Toxoplasma gondii* - **Toxoplasmosis** can cause fever and rash, especially in congenital infections or immunocompromised individuals. - However, it does not lead to **owl's eye inclusions** in urinary cells, which are pathognomonic for CMV. *Infectious mononucleosis caused by Epstein-Barr virus* - **Infectious mononucleosis** commonly presents with fever, fatigue, and lymphadenopathy, sometimes with a rash. - **Epstein-Barr virus (EBV)** infection does not produce cells with an **owl's eye appearance** in the urine; that is specific to CMV.
Question 8: Which vitamin deficiency is most commonly associated with rickets in children?
- A. Vitamin A
- B. Vitamin C
- C. Vitamin D (Correct Answer)
- D. Vitamin K
Explanation: ***Vitamin D*** - **Vitamin D** plays a crucial role in the absorption of **calcium** and **phosphate**, which are essential for proper **bone mineralization**. - A deficiency leads to impaired mineralization of newly formed bone matrix, resulting in soft, weak bones characteristic of **rickets** in children and **osteomalacia** in adults. *Vitamin A* - **Vitamin A** is primarily involved in **vision**, immune function, and cell growth and differentiation. - While essential for health, its deficiency is not directly linked to the skeletal deformities seen in rickets. *Vitamin C* - **Vitamin C** is vital for **collagen synthesis**, a key component of connective tissues, skin, and bone matrix. - Its deficiency causes **scurvy**, characterized by bleeding gums, poor wound healing, and joint pain, not the bone deformities of rickets. *Vitamin K* - **Vitamin K** is essential for **blood coagulation** and plays a role in bone metabolism through the carboxylation of certain bone proteins like **osteocalcin**. - However, its deficiency primarily leads to bleeding disorders and does not cause rickets.
Question 9: A 2-year-old child with a history of eczema presents with a red, scaly rash around the mouth and extremities. A dietary history reveals excessive consumption of cow's milk. What nutritional deficiency is most likely?
- A. Zinc deficiency (Correct Answer)
- B. Iron deficiency
- C. Vitamin D deficiency
- D. Vitamin C deficiency
Explanation: ***Zinc deficiency*** - The combination of **eczema**, perioral and acral **dermatitis** (red, scaly rash around the mouth and extremities), and a diet rich in **cow's milk** in a 2-year-old strongly points to zinc deficiency. - Cow's milk can inhibit **zinc absorption**, and infants with eczema may have increased zinc demands or impaired absorption. *Iron deficiency* - While common in toddlers, especially with high cow's milk intake, **iron deficiency** primarily manifests as **anemia**, pallor, and fatigue, not a characteristic rash. - It does not typically cause the specific **dermatitis** described. *Vitamin D deficiency* - Primarily linked to **rickets** in children, causing bone deformities and growth delays. - Does not present with a **red, scaly rash** around the mouth and extremities. *Vitamin C deficiency* - Leads to **scurvy**, characterized by swollen, bleeding gums, perifollicular hemorrhages, and poor wound healing. - The described **dermatological symptoms** are not typical of vitamin C deficiency.
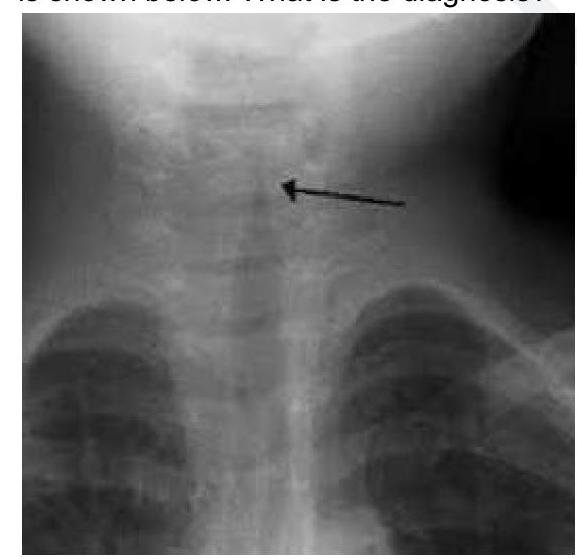
Question 10: A 2 year child presented with low grade fever and stridor. What is the likely diagnosis?
- A. Acute Laryngotracheobronchitis (Correct Answer)
- B. Acute Bacterial Tracheitis
- C. Acute Epiglottitis
- D. Foreign Body aspiration
Explanation: ***Acute Laryngotracheobronchitis*** - The combination of **low-grade fever** and **stridor** in a 2-year-old child strongly suggests **croup**, which is medically known as acute laryngotracheobronchitis. - Croup is characterized by **inflammation** of the larynx, trachea, and bronchi, often presenting with a **barking cough** and inspiratory stridor. The X-ray image would show the characteristic **steeple sign**. *Acute Bacterial Tracheitis* - This is a more severe bacterial infection that can present with stridor but typically shows **higher fever**, **toxic appearance**, and rapid clinical deterioration. - Unlike croup, bacterial tracheitis patients appear **more ill** and may have **purulent secretions** requiring more aggressive management. *Acute Epiglottitis* - A serious condition characterized by **rapid onset of high fever**, **dysphagia**, drooling, and a **"tripod" position**, which are not indicated by the given symptoms. - The stridor in epiglottitis is typically quieter and may indicate more severe airway obstruction compared to the characteristic stridor of croup. *Foreign Body aspiration* - While foreign body aspiration can cause stridor, it is typically an **acute event** with a sudden onset of choking, coughing, and respiratory distress. - There is no mention of a choking episode or sudden onset, and a low-grade fever is less typical for an uncomplicated foreign body aspiration.