All (135)Anatomy (8)Anesthesiology (1)Biochemistry (9)Community Medicine (8)Dental (2)Dermatology (2)ENT (2)Forensic Medicine (3)Internal Medicine (20)Microbiology (7)Obstetrics and Gynecology (12)Ophthalmology (4)Orthopaedics (4)Pathology (6)Pediatrics (10)Pharmacology (13)Physiology (5)Psychiatry (2)Psychiatry (3)Radiology (1)Surgery (13)
Q101
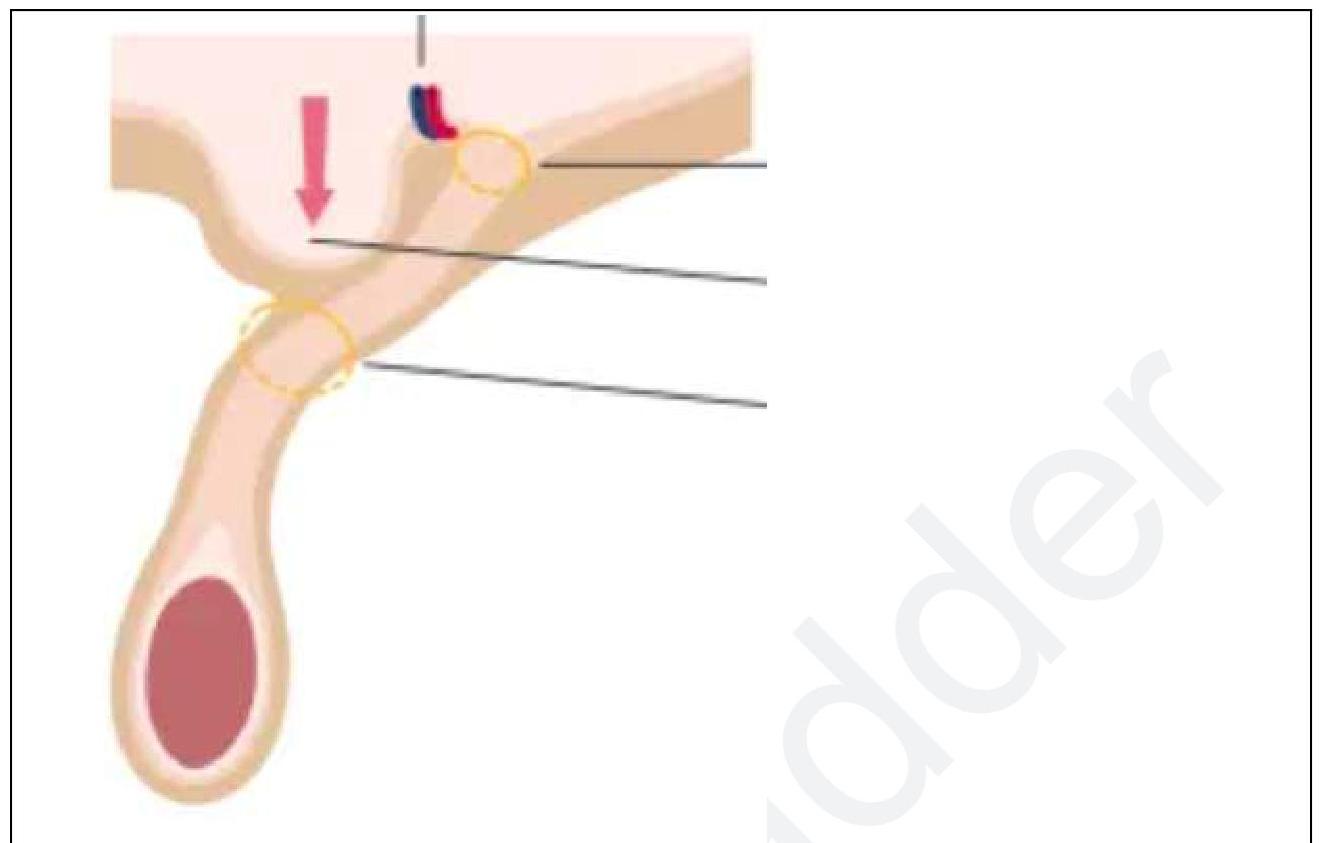
Which muscle is attached to the disc of the temporomandibular joint?