NEET-PG 2023 — Internal Medicine
30 Previous Year Questions with Answers & Explanations
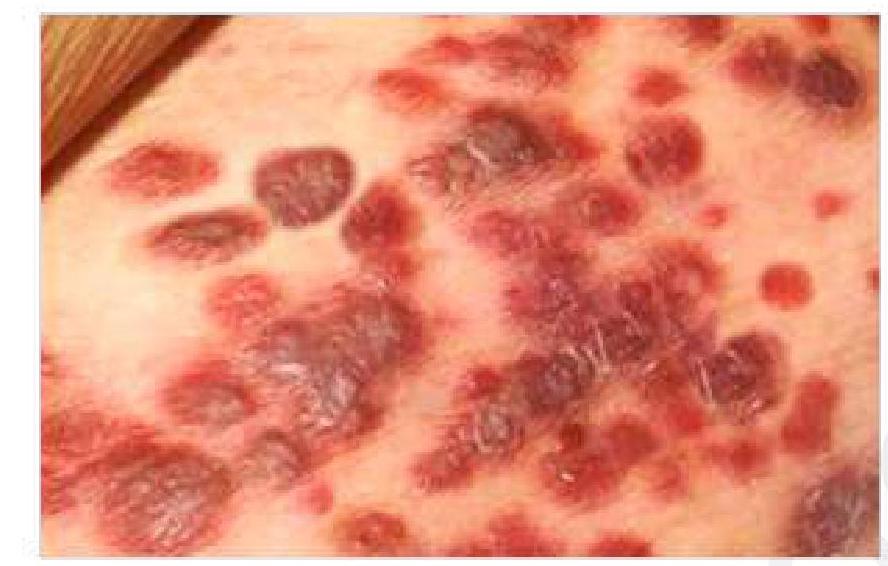
A 50-year-old HIV-positive patient presents with a painless, purple lesion on the skin. What is the most likely diagnosis?
In which of the following conditions is neoadjuvant chemotherapy not typically used?
Which of the following is a potential complication of blood transfusion?
A patient complains of loss of visual acuity, deafness, and enlargement of the maxilla.

What type of murmur is most likely associated with a patient presenting with elevated JVP, large v-waves, and a loud systolic murmur?
A farmer was sleeping in the field, and he felt a sting on his leg. He saw something moving away quickly. He then got drowsy and was taken to the hospital. He developed pain around the site and continued to bleed profusely from the wound site. The wound became red with blisters. Which of the following is the most likely cause?
A bronchial asthma patient on inhalational steroids presented with white patchy lesions on the tongue and buccal mucosa. What condition is likely to be present in this patient?
A patient with a history of alcohol dependence syndrome presents with sudden and unintentional weight loss. What is the most likely diagnosis?
A chronic alcoholic is brought to the emergency department with confusion, ataxia, and painful eye movements, including nystagmus. The 6th cranial nerve is also involved. What is the likely diagnosis?
In a patient presented with a fever and a positive filarial antigen test, what is the next appropriate method of management?
NEET-PG 2023 - Internal Medicine NEET-PG Practice Questions and MCQs
Question 1: A 50-year-old HIV-positive patient presents with a painless, purple lesion on the skin. What is the most likely diagnosis?
- A. Kaposi's sarcoma (Correct Answer)
- B. Squamous cell carcinoma
- C. Malignant melanoma
- D. Basal cell carcinoma
Explanation: ***Kaposi's sarcoma*** - The presentation of **painless, purple skin lesions** in an **HIV-positive patient** is highly characteristic of Kaposi's sarcoma. - This is a vascular tumor caused by **Human Herpesvirus 8 (HHV-8)**, often seen in immunocompromised individuals. *Malignant melanoma* - Malignant melanoma typically presents as a **dark, irregularly shaped lesion** with varying colors and often exhibits change in size, shape, or color over time (**ABCDEs of melanoma**). - While it can be purple or dark, the multiple, widespread nature and association with HIV points away from typical melanoma. *Squamous cell carcinoma* - Squamous cell carcinoma usually presents as a **red, scaly patch, nodule, or an open sore** that doesn't heal, often found in sun-exposed areas. - It is not typically described as a painless purple lesion, and while HIV patients have increased risk, the lesion morphology is more consistent with Kaposi's. *Basal cell carcinoma* - Basal cell carcinoma commonly appears as a **pearly or waxy bump**, a **flat, flesh-colored lesion**, or a **brown, scar-like lesion**, often with a rolled border and telangiectasias. - Unlike the description, it is not typically purple and painless, and while common, the clinical picture with HIV is not classic for BCC.
Question 2: In which of the following conditions is neoadjuvant chemotherapy not typically used?
- A. Thyroid cancer (Correct Answer)
- B. Breast cancer
- C. Esophageal cancer
- D. Lung cancer
Explanation: ***Thyroid cancer*** - **Neoadjuvant chemotherapy** is generally **not used** for the treatment of thyroid cancer, as it is primarily managed with surgery, radioactive iodine, and thyroid hormone suppression [1]. - Most thyroid cancers, especially differentiated types like **papillary** and **follicular carcinoma**, are not highly sensitive to conventional chemotherapy [1]. *Breast cancer* - **Neoadjuvant chemotherapy** is a common approach in **locally advanced breast cancer** to downstage tumors, improve surgical outcomes, and assess treatment response. - It may also be used in cases of **inflammatory** or certain aggressive subtypes like **triple-negative** breast cancer. *Esophageal cancer* - **Neoadjuvant chemotherapy**, often combined with **radiation** (chemoradiotherapy), is a standard treatment for **locally advanced esophageal cancer**. - Its purpose is to **downstage** the tumor, reduce invasiveness, and improve surgical resectability and survival rates. *Lung cancer* - **Neoadjuvant chemotherapy** is frequently employed for **locally advanced non-small cell lung cancer** (NSCLC) to reduce tumor size and extent before surgical resection. - This approach aims to improve the likelihood of a complete surgical removal and overall prognosis.
Question 3: Which of the following is a potential complication of blood transfusion?
- A. Hyponatremia
- B. Hypercalcemia
- C. Increased serum albumin
- D. Hyperkalemia (Correct Answer)
Explanation: ***Hyperkalemia*** - Stored red blood cells can release **intracellular potassium** into the storage solution, leading to elevated potassium levels in transfused blood. - Rapid or massive transfusions deliver a significant potassium load, potentially causing **cardiac arrhythmias**. *Hyponatremia* - This is generally not a direct complication of blood transfusions; instead, blood products themselves contain electrolytes, and massive transfusion can disrupt electrolyte balance, but usually not to cause hyponatremia. - Volume overload from transfusion could dilute existing electrolytes, but most commonly, other electrolyte imbalances such as hyperkalemia or hypocalcemia occur. *Hypercalcemia* - Often, the opposite, **hypocalcemia**, is a complication of massive transfusion due to **citrate toxicity**. - Citrate, an anticoagulant in transfused blood, chelates calcium, reducing free calcium levels in the recipient. *Increased serum albumin* - Blood transfusions primarily administer **red blood cells**, plasma, or platelets, not typically albumin in amounts that would significantly increase serum albumin levels in the absence of an albumin-specific infusion [1]. - Low albumin (hypoalbuminemia) is a common finding in critically ill patients, and a blood transfusion usually doesn't correct this unless plasma or albumin is specifically administered [1].
Question 4: A patient complains of loss of visual acuity, deafness, and enlargement of the maxilla.
- A. Fibrous dysplasia
- B. Osteogenesis imperfecta
- C. Paget's disease (Correct Answer)
- D. Osteomalacia
Explanation: ***Paget's disease*** [1] - Characterized by abnormal **bone remodeling**, leading to an increase in bone size and deformity, particularly in the **maxilla**, causing enlargement [1]. - Associated with complications such as **loss of visual acuity** (due to involvement of the skull) and **deafness** from auditory canal changes [1][2], making this the most fitting diagnosis. *Fibrous dysplasia* - Typically presents with **fibrous replacement** of bone, not specifically causing deafness or visual acuity loss. - Customarily involves the **classic "ground glass" appearance** on imaging, not the structural enlargement seen in Paget's disease. *Osteogenesis imperfecta* - Mainly causes **brittle bones** and frequent fractures, not associated with **maxillary enlargement** or changes in auditory function. - Rarely causes visual acuity loss, which is not a feature of this condition. *Osteomalacia* - Primarily characterized by **softening of bones** due to vitamin D deficiency, leading to weakness rather than structural changes like maxillary enlargement. - Symptoms like **bone pain** or **muscle weakness** occur, but not specifically loss of auditory function or visual acuity. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Bones, Joints, and Soft Tissue Tumors, pp. 1192-1194. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Osteoarticular And Connective Tissue Disease, pp. 669-670.
Question 5: What type of murmur is most likely associated with a patient presenting with elevated JVP, large v-waves, and a loud systolic murmur?
- A. Functional murmur
- B. Tricuspid stenosis
- C. Pulmonary stenosis
- D. Tricuspid regurgitation (Correct Answer)
Explanation: ***Tricuspid regurgitation*** - **Elevated JVP** with prominent **v-waves** and a **loud systolic murmur** are classic findings for tricuspid regurgitation. [1] The large v-waves are due to blood regurgitating into the right atrium during ventricular systole. - The murmur is typically **holosystolic** and may increase with inspiration (Carvallo's sign). *Functional murmur* - Functional murmurs are generally **benign**, not associated with significant hemodynamic compromise, and rarely present with elevated JVP or prominent v-waves. - They are typically **soft**, early or mid-systolic, and often change intensity with position. *Tricuspid stenosis* - Tricuspid stenosis would cause an **elevated JVP**, but the prominent wave would be an **a-wave** (due to increased right atrial pressure during atrial contraction), not a v-wave. - The murmur associated with tricuspid stenosis is a **diastolic rumble**, not a systolic murmur. [3] *Pulmonary stenosis* - Pulmonary stenosis presents with a **systolic ejection murmur** at the upper left sternal border and can cause elevated JVP due to right ventricular hypertrophy and failure. [2] - However, it typically does not cause prominent **v-waves** in the JVP, as the issue is outflow obstruction from the right ventricle, not regurgitation into the right atrium.
Question 6: A farmer was sleeping in the field, and he felt a sting on his leg. He saw something moving away quickly. He then got drowsy and was taken to the hospital. He developed pain around the site and continued to bleed profusely from the wound site. The wound became red with blisters. Which of the following is the most likely cause?
- A. Viper bite (Correct Answer)
- B. Cobra bite
- C. Wasp sting
- D. Scorpion sting
Explanation: ***Viper bite*** - **Viper venom** is predominantly **hemotoxic**, causing local tissue damage (pain, redness, blistering, bleeding) and systemic effects like **coagulopathy**, leading to profuse bleeding [1]. - The rapid onset of drowsiness, local pain, bleeding, and blistering are classic signs of **viper envenomation** [1]. *Cobra bite* - **Cobra venom** is primarily **neurotoxic**, leading to **flaccid paralysis**, ptosis, and respiratory failure, rather than significant local tissue destruction or profuse bleeding [1]. - While local swelling and pain may occur, extensive blistering and significant bleeding are less characteristic compared to viper bites [1]. *Wasp sting* - A **wasp sting** causes localized pain, swelling, and redness, and may lead to an **anaphylactic reaction** in sensitive individuals [2]. - It does not typically cause profuse, prolonged bleeding or extensive blistering at the wound site as seen here [2]. *Scorpion sting* - **Scorpion stings** typically cause intense localized pain, paresthesias, and sometimes systemic symptoms like hypertension, tachycardia, and neurological effects [3]. - They do not typically cause widespread **hemorrhagic symptoms** or significant local blistering and extensive bleeding as described [3].
Question 7: A bronchial asthma patient on inhalational steroids presented with white patchy lesions on the tongue and buccal mucosa. What condition is likely to be present in this patient?
- A. Oral lichen planus
- B. Aphthous ulcers
- C. Oral leukoplakia
- D. Oral candidiasis (Correct Answer)
Explanation: **Oral candidiasis** - **Inhaled corticosteroids** can suppress the local immune response in the oral cavity, creating an environment conducive to the overgrowth of *Candida albicans*. - The classic presentation includes **white patchy lesions** on the tongue and buccal mucosa, which can often be scraped off. *Oral lichen planus* - Characterized by **reticular (Wickham's striae)**, papular, or erosive lesions, which are often bilateral and symmetric [1]. - While it can present with white lesions, they are typically not easily scraped off and are not primarily associated with inhaled corticosteroid use [1]. *Aphthous ulcers* - These are typically **painful, solitary, or multiple ulcers** with a red halo and a yellowish-gray center [2]. - They are distinct from widespread white patchy lesions and are not directly caused by inhaled corticosteroid use [2]. *Oral leukoplakia* - Defined as a **white patch or plaque** on the oral mucosa that cannot be characterized clinically or pathologically as any other disease, and which is not removable by scraping. - It is often associated with tobacco use and alcohol consumption, and carries a risk of malignancy; it does not typically appear as a direct side effect of inhaled corticosteroids.
Question 8: A patient with a history of alcohol dependence syndrome presents with sudden and unintentional weight loss. What is the most likely diagnosis?
- A. Hepatic adenoma
- B. Cholangiocarcinoma
- C. Hepatocellular carcinoma (Correct Answer)
- D. Alcoholic hepatitis
Explanation: ***Hepatocellular carcinoma*** - The **alpha-fetoprotein (AFP)** level of **600 ng/mL** is significantly elevated, suggesting a diagnosis of hepatocellular carcinoma, especially in a patient with a history of **alcohol dependence syndrome** [1]. - The **AST/ALT ratio of 0.5** indicates significant liver damage, commonly seen in chronic liver disease leading to **hepatocellular cancer**. *Alcoholic hepatitis* - Typically presents with **elevated AST and ALT**, usually with a ratio >2:1, which is not the case here [2]. - May cause weight loss, as alcoholic patients often lose weight due to self-neglect and poor dietary intake, but the **elevated AFP** is not characteristic of merely alcoholic hepatitis [3]. *Cholangiocarcinoma* - This type of cancer primarily presents with **biliary obstruction** symptoms, such as jaundice, which is not indicated here given **normal bilirubin levels**. - Does not typically lead to such high levels of **AFP**, making it less likely with the provided lab results. *Hepatic adenoma* - More commonly associated with **oral contraceptive use** or anabolic steroid use, not primarily alcohol dependence. - AFP levels are usually normal or only mildly elevated in hepatic adenoma, making this option less viable with an **AFP level of 600 ng/mL**.
Question 9: A chronic alcoholic is brought to the emergency department with confusion, ataxia, and painful eye movements, including nystagmus. The 6th cranial nerve is also involved. What is the likely diagnosis?
- A. Wernicke's encephalopathy (Correct Answer)
- B. Korsakoff psychosis
- C. Delirium tremens
- D. De Clerambault syndrome
Explanation: ***Wernicke's encephalopathy*** - This diagnosis aligns perfectly with the classic triad of **confusion, ataxia, and ophthalmoplegia** (manifested as painful eye movements, nystagmus, and 6th cranial nerve involvement) in the setting of chronic alcoholism [1], [2]. - It is caused by **thiamine (vitamin B1) deficiency**, common in chronic alcoholics due to malnutrition and impaired absorption [1]. *Korsakoff psychosis* - This condition is typically a **later complication** of Wernicke's encephalopathy, characterized by profound **anterograde and retrograde amnesia**, confabulation, and apathy [2]. - While an alcoholic patient might develop this, the immediate presentation with acute confusion, ataxia, and cranial nerve signs points to Wernicke's encephalopathy being the more acute and primary diagnosis in this scenario. *Delirium tremens* - This is a severe form of **alcohol withdrawal**, typically occurring 48-96 hours after the last drink, and is characterized by **global confusion, hallucinations (often visual), severe autonomic instability** (tachycardia, hypertension, fever, sweating), and seizures [3]. - While confusion is present, the specific neurological signs like ataxia and ophthalmoplegia are not typical of delirium tremens. *De Clerambault syndrome* - Also known as **erotomania**, this is a rare delusional disorder where an individual has a fixed, false belief that another person, usually of higher social status, is in love with them. - This is a **psychiatric disorder** with no relation to the neurological symptoms or alcohol-related complications described in the patient.
Question 10: In a patient presented with a fever and a positive filarial antigen test, what is the next appropriate method of management?
- A. Bone marrow biopsy
- B. DEC provocation test
- C. Detection of microfilariae in the blood smear (Correct Answer)
- D. Ultrasound of the scrotum
Explanation: ***Detection of microfilariae in the blood smear*** - A positive **filarial antigen test** indicates the presence of adult worms, and the next step is to confirm active infection by identifying **microfilariae**. [1] - **Nocturnal blood samples** are crucial because microfilariae of *Wuchereria bancrofti* and *Brugia malayi* exhibit **nocturnal periodicity**, meaning they are most abundant in peripheral blood between 10 PM and 2 AM. [1] *Bone marrow biopsy* - This procedure is typically used to diagnose **hematological disorders**, such as leukemia or lymphoma, or investigate causes of unexplained fever, but it is not indicated for filariasis. - While filariasis can rarely lead to **eosinophilia**, a bone marrow biopsy is not a diagnostic tool for filarial infection itself. *DEC provocation test* - The **diethylcarbamazine (DEC) provocation test** is used to bring out microfilariae into the peripheral blood during the daytime for species that exhibit nocturnal periodicity. [1] - However, it carries a risk of severe adverse reactions due to rapid killing of microfilariae, especially in cases of heavy infection, and is generally avoided when antigen tests are positive. [1] *Ultrasound of the scrotum* - Scrotal ultrasound can detect the characteristic "filarial dance sign" (motile adult worms) in the **lymphatic vessels of the scrotum and epididymis**, confirming lymphatic filariasis. [2] - While useful for assessing advanced disease manifestations like **hydrocele**, it does not quantify microfilaremia or replace the need for microscopic confirmation of circulating microfilariae to guide treatment.