NEET-PG 2023 — Anatomy
8 Previous Year Questions with Answers & Explanations
What embryological failure leads to the formation of a double aortic arch?
What anatomical structure is formed after the obliteration of the umbilical vein?
A female presents with loss of vision in the right halves of both eyes. Where is the lesion located in the optic pathway?
The given histology image is of which structure?
A patient is brought to the OPD by his wife, complaining about difficulty expressing emotions and lack of participation in daily activities. On examination, resting tremors and rigidity are noted. Given the possible diagnosis, which part of the brain is affected in this patient?
Injury at which of the following marked sites on the leg causes failure of dorsiflexion?

During acute tonsillitis, referred pain from the tonsil to the middle ear occurs via which nerve?
Which of the following is true about nerve injuries?
NEET-PG 2023 - Anatomy NEET-PG Practice Questions and MCQs
Question 1: What embryological failure leads to the formation of a double aortic arch?
- A. Failure of neural crest cell migration
- B. Abnormal development of the ductus arteriosus
- C. Failure of the 6th aortic arch to develop
- D. Failure of regression of the right dorsal aorta (Correct Answer)
Explanation: **Failure of regression of the right dorsal aorta** - A double aortic arch results from the **persistence of both right and left aortic arches** that encircle the trachea and esophagus, forming a vascular ring [1]. - In normal development, the **distal right dorsal aorta** (the segment between the right subclavian artery origin and the descending aorta) regresses, leaving only the left arch as the definitive aortic arch. - When this regression fails, both the right and left arches persist, creating a **complete vascular ring** around the trachea and esophagus, which can cause compression symptoms [1]. - This is one of the most common causes of a **symptomatic vascular ring** in infants [1]. *Failure of the 6th aortic arch to develop* - The 6th aortic arches contribute to the **pulmonary arteries** and the **ductus arteriosus**. Their failure to develop would lead to pulmonary circulation anomalies, not a double aortic arch. - This failure is associated with conditions like **pulmonary atresia** or **absent pulmonary artery**. *Abnormal development of the ductus arteriosus* - The ductus arteriosus is derived from the **distal part of the left 6th aortic arch**. Abnormal development typically leads to conditions like **patent ductus arteriosus (PDA)**. - This would not cause two complete aortic arches to persist around the trachea and esophagus. - While a right-sided ductus can be part of some vascular ring anomalies, it is not the primary cause of double aortic arch. *Failure of neural crest cell migration* - Neural crest cells are crucial for the **septation of the truncus arteriosus** and the formation of the aorticopulmonary septum. - Failure of neural crest cell migration is associated with conotruncal heart defects such as **Tetralogy of Fallot**, **Persistent truncus arteriosus**, or **Transposition of the Great Arteries**, not a double aortic arch. - Double aortic arch is primarily a failure of normal regression, not a neural crest cell defect.
Question 2: What anatomical structure is formed after the obliteration of the umbilical vein?
- A. Ligamentum venosum
- B. Ligamentum arteriosum
- C. Medial umbilical ligament
- D. Round ligament of the liver (ligamentum teres) (Correct Answer)
Explanation: ***Round ligament of the liver (ligamentum teres)*** - The **umbilical vein** carries oxygenated blood from the placenta to the fetus during development [1]. - After birth, the umbilical vein obliterates and forms the **round ligament of the liver**, also known as the **ligamentum teres hepatis**. *Ligamentum venosum* - This structure is the obliterated remnant of the **ductus venosus**, which shunted blood from the umbilical vein to the inferior vena cava, bypassing the fetal liver [1]. - It is located in a fissure on the posterior surface of the liver, separate from the round ligament. *Ligamentum arteriosum* - This ligament is the remnant of the **ductus arteriosus**, a fetal blood vessel connecting the pulmonary artery to the aorta. - Its obliteration allows blood to flow through the lungs after birth. *Medial umbilical ligament* - This ligament is formed from the obliterated **umbilical arteries**, which carry deoxygenated blood from the fetus back to the placenta. - There are two medial umbilical ligaments, one from each umbilical artery.
Question 3: A female presents with loss of vision in the right halves of both eyes. Where is the lesion located in the optic pathway?
- A. Left optic tract (Correct Answer)
- B. Optic radiation
- C. Optic chiasma
- D. Right optic tract
Explanation: Left optic tract - A lesion in the **left optic tract** causes **right homonymous hemianopsia**, meaning loss of vision in the right halves of both eyes [1]. - This is because the left optic tract carries visual information from the **nasal retina of the right eye** and the **temporal retina of the left eye**, both of which process the right visual field [1]. *Optic radiation* - A lesion in the optic radiation would also cause a **homonymous hemianopsia** but depending on the specific location within the radiation, it could result in a **quadrantanopia** (loss of a quarter visual field) rather than a complete hemianopsia. - The optic radiation projects from the **lateral geniculate nucleus** to the **visual cortex**, and damage here affects the post-chiasmatic visual pathway [1]. *Optic chiasma* - A lesion at the **optic chiasma** typically results in **bitemporal hemianopsia**, which is the loss of vision in the **temporal halves of both eyes** [1]. - This occurs because the **crossing nasal fibers** from both eyes, which carry information from the temporal visual fields, are affected [1]. *Right optic tract* - A lesion in the **right optic tract** would result in **left homonymous hemianopsia**, meaning loss of vision in the **left halves of both eyes** [1]. - This is due to the right optic tract carrying fibers from the **nasal retina of the left eye** and the **temporal retina of the right eye**, both of which process the left visual field [1].
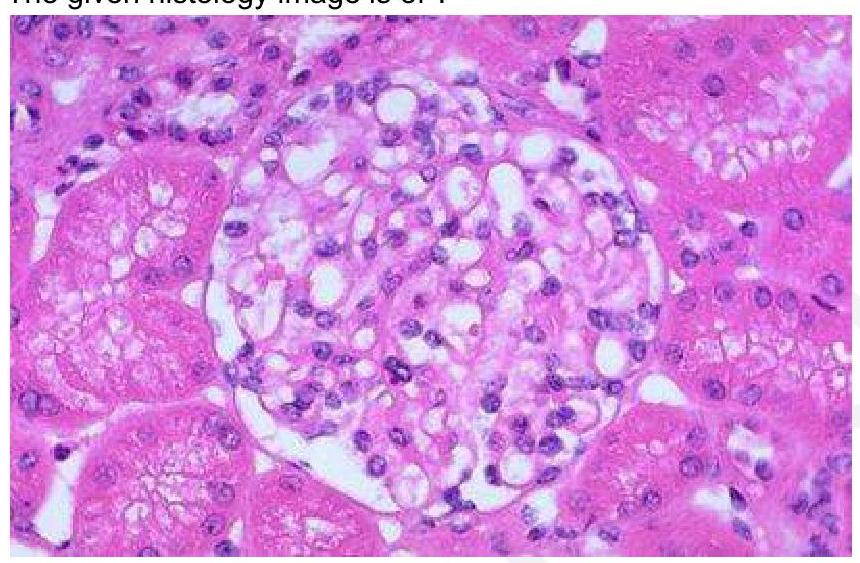
Question 4: The given histology image is of which structure?
- A. Pancreatic islet cells
- B. Hassall's corpuscles
- C. Glomerulus (Correct Answer)
- D. Leydig cells in the testis
Explanation: ***Glomerulus*** - The glomerulus is characterized by a **tuft of capillaries** surrounded by Bowman's capsule, responsible for filtration in the kidney [1]. - Histological examination typically shows a **dense network of capillaries** and **mesangial cells**, which are distinct features of the glomeruli [1]. *Hassall's corpuscles* - Found in the **thymus**, they are round structures composed of epithelial cells, crucial in T-cell maturation. - Histologically, they present as concentric layers of **epithelial cells** and are not found in the kidney. *Leydig cells of testis* - Located in the **interstitial tissue** of the testes, these cells produce testosterone and are typically larger than glomerular cells. - They are characterized by their **eosinophilic cytoplasm** and round nuclei, differing markedly from the structures found in the glomerulus. *Pancreatic islet cells* - Islet cells are involved in **hormone production**, predominantly insulin and glucagon, and are located in the pancreas. - Histologically, they appear as small clusters dispersed among **exocrine pancreas**, which is different from the highly organized structure of the glomerulus. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 522-523.
Question 5: A patient is brought to the OPD by his wife, complaining about difficulty expressing emotions and lack of participation in daily activities. On examination, resting tremors and rigidity are noted. Given the possible diagnosis, which part of the brain is affected in this patient?
- A. Basal ganglia (Correct Answer)
- B. Hippocampus
- C. Cerebellum
- D. Premotor cortex
Explanation: **Basal ganglia (Correct)** - The symptoms described—**resting tremors**, **rigidity**, difficulty expressing emotions, and lack of participation—are classic features of **Parkinson's disease**, which is characterized by the degeneration of dopaminergic neurons in the **substantia nigra**, a component of the basal ganglia [1]. - The basal ganglia play a crucial role in motor control, learning, and emotion, and their dysfunction leads to the characteristic motor and non-motor symptoms observed [2]. *Hippocampus (Incorrect)* - The hippocampus is primarily involved in **memory formation** and spatial navigation. - Damage to the hippocampus typically results in **amnesia** or difficulties with new learning, not motor symptoms like tremors or rigidity [3]. *Cerebellum (Incorrect)* - The cerebellum is responsible for **coordination**, balance, and fine motor control [2]. - **Cerebellar dysfunction** typically manifests as **ataxia**, dysmetria, and intention tremors, which differ from the resting tremors and rigidity seen in this patient. *Premotor cortex (Incorrect)* - The premotor cortex is involved in the planning and preparation of movements, as well as the control of trunk and proximal limb muscles. - While it contributes to motor control, its primary dysfunction does not typically cause the combination of **resting tremors** and **rigidity** characteristic of Parkinson's disease.
Question 6: Injury at which of the following marked sites on the leg causes failure of dorsiflexion?
- A. Anterior aspect of the thigh (site 1)
- B. Medial aspect of the leg (site 4)
- C. Lateral aspect of the leg (site 3) (Correct Answer)
- D. Posterior aspect of the thigh (site 2)
Explanation: ***Lateral aspect of the leg (site 3)*** - Site 3 points to the **fibula head** and the adjacent region on the lateral aspect of the leg. This is the anatomical location where the **common fibular nerve (peroneal nerve)** wraps around. - The common fibular nerve innervates the muscles responsible for **dorsiflexion** and eversion of the foot. Damage to this nerve, often due to trauma at the fibular neck, leads to **foot drop** and an inability to dorsiflex the foot. *Anterior aspect of the thigh (site 1)* - Site 1 points to the distal femur, which is part of the thigh. Nerves in the anterior thigh (e.g., **femoral nerve**) primarily control hip flexion and knee extension. - Damage here would affect movements of the hip and knee, not directly causing failure of dorsiflexion of the foot. *Medial aspect of the leg (site 4)* - Site 4 points to the medial tibia. This area is associated with the **tibial nerve** and saphenous nerve, which primarily innervate muscles for plantarflexion and inversion of the foot, or provide sensory innervation. - Injury to the tibial nerve would result in an inability to plantarflex and invert the foot, not dorsiflexion. *Posterior aspect of the thigh (site 2)* - Site 2 points to the posterior aspect of the thigh, which is the region for the hamstrings. The **sciatic nerve** and its branches (tibial and common fibular) pass through this region. - While the common fibular nerve originates from the sciatic nerve in the posterior thigh, an injury at this level would likely cause more widespread motor and sensory deficits than isolated dorsiflexion failure, and site 3 is a more common and specific site for common fibular nerve injury isolated to foot drop.
Question 7: During acute tonsillitis, referred pain from the tonsil to the middle ear occurs via which nerve?
- A. Facial nerve
- B. Glossopharyngeal nerve (Correct Answer)
- C. Trigeminal nerve
- D. Vagus nerve
Explanation: ***Glossopharyngeal nerve*** - The **glossopharyngeal nerve (CN IX)** provides sensory innervation to the palatine tonsil via its tonsillar branches - CN IX also supplies the middle ear via the **tympanic nerve (Jacobson's nerve)**, which forms the tympanic plexus - This shared sensory pathway explains **referred otalgia** (ear pain) during acute tonsillitis - Inflammation of the tonsil stimulates CN IX, and the brain misinterprets this as pain from the middle ear *Facial nerve* - The **facial nerve (CN VII)** primarily provides motor innervation to muscles of facial expression and taste to the anterior two-thirds of the tongue - While it has a small sensory component (nervus intermedius) for the external auditory canal, it does not innervate the tonsil - Cannot serve as the pathway for referred pain from tonsil to middle ear *Trigeminal nerve* - The **trigeminal nerve (CN V)** provides sensory innervation to the face, anterior scalp, and oral cavity - Does not innervate the palatine tonsil or the middle ear cavity - Not involved in tonsillar referred otalgia *Vagus nerve* - The **vagus nerve (CN X)** provides sensory innervation to parts of the pharynx, larynx, and external auditory canal (via Arnold's nerve) - While it contributes to pharyngeal sensation, the **glossopharyngeal nerve is the primary pathway** for referred otalgia from tonsillar inflammation due to its direct innervation of both the tonsil and middle ear
Question 8: Which of the following is true about nerve injuries?
- A. Froment sign seen in median nerve palsy is due to Flexor pollicis longus action
- B. All lumbricals are supplied by median nerve
- C. Waenburg sign is seen in median nerve palsy
- D. Median nerve is also named as labourer's nerve (Correct Answer)
Explanation: ***Median nerve is also named as labourer's nerve*** - The median nerve is sometimes called the "laborer's nerve" because it innervates many of the muscles essential for **fine motor control** and **dexterous hand movements** predominantly used in manual labor. [1] - It supplies most of the **flexors in the forearm** and several intrinsic hand muscles, making it crucial for a strong grip and coordinated hand actions. [1] *Froment sign seen in median nerve palsy is due to Flexor pollicis longus action* - **Froment's sign** is observed in **ulnar nerve palsy**, not median nerve palsy. - It occurs when the adductor pollicis is weak, and the **flexor pollicis longus** (median nerve-innervated) compensates by hyperflexing the interphalangeal joint of the thumb to grasp an object. *All lumbricals are supplied by median nerve* - The **first two lumbricals** (from the radial side) are typically supplied by the **median nerve**. [1] - The **third and fourth lumbricals** (from the ulnar side) are supplied by the **ulnar nerve**. [1] *Waenburg sign is seen in median nerve palsy* - There is no widely recognized clinical sign called "Waenburg sign" associated with median nerve palsy. - Common signs of **median nerve palsy** include **ape hand deformity**, **hand of benediction**, and sensory loss in the radial three and a half digits. [1]