NEET-PG 2021 — Surgery
15 Previous Year Questions with Answers & Explanations
A 35-year-old male presents with posterior epistaxis. Conservative management including nasal packing to stop the bleeding was unsuccessful. What is the next step in the management of this patient?
Which of the following is a common topical use of the medicine shown in the image?

A child who underwent a tonsillectomy started bleeding while lying in the ward post-operatively. Which of the following is the most appropriate management step?
What surgery is shown here in the image?
A patient presents with upper limb swelling after undergoing a modified radical mastectomy (MRM). What is the most likely cause?
Which of the following is the most commonly performed repair for a direct inguinal hernia?
A patient presents with breathlessness and decreased air entry into the right lung following a road traffic accident (RTA) and is hypotensive. What is the next step in management?
After a total thyroidectomy, the surgeon is unable to extubate the patient, who shows cyanosis and respiratory distress. What is the most likely cause of the inability to extubate?
Asymptomatic varicose veins would fall under which category of the CEAP classification system?
Which nerve is most commonly injured during submandibular gland surgery?
NEET-PG 2021 - Surgery NEET-PG Practice Questions and MCQs
Question 1: A 35-year-old male presents with posterior epistaxis. Conservative management including nasal packing to stop the bleeding was unsuccessful. What is the next step in the management of this patient?
- A. Internal carotid artery (ICA) ligation
- B. Maxillary artery ligation
- C. External carotid artery (ECA) ligation
- D. Endoscopic sphenopalatine artery ligation (Correct Answer)
Explanation: ***Endoscopic sphenopalatine artery ligation*** - **Sphenopalatine artery ligation** is the most common surgical intervention for **posterior epistaxis** that is refractory to conservative management (e.g., nasal packing). - It is highly effective because the sphenopalatine artery is the major blood supply to the **posterior nasal cavity**. *Internal carotid artery (ICA) ligation* - **ICA ligation** is rarely performed for epistaxis due to the risk of **neurological complications**, such as stroke. - The ICA primarily supplies the brain, and its contribution to nasal bleeding is indirect and not typically the primary source. *Maxillary artery ligation* - The **maxillary artery** is the parent artery of the sphenopalatine artery, but ligating it more proximally carries a higher risk of complications and is less precise. - Due to the deep anatomical location, this approach is more invasive and technically challenging than sphenopalatine artery ligation. *External carotid artery (ECA) ligation* - **ECA ligation** is a more proximal and less selective procedure than sphenopalatine artery ligation, meaning other vessels may be ligated unnecessarily. - While it can reduce blood flow, it may not be as effective as direct sphenopalatine artery ligation for controlling severe posterior epistaxis, as collateral blood flow can still occur.
Question 2: Which of the following is a common topical use of the medicine shown in the image?
- A. Rhino cerebral mucormycosis
- B. Inlay type I myringoplasty
- C. Post-adenoidectomy to control bleeding (Correct Answer)
- D. Subglottic stenosis
Explanation: ***Post-adenoidectomy to control bleeding*** - The image shows **Neo-Synephrine (phenylephrine)**, a potent **alpha-adrenergic agonist** that causes **vasoconstriction**. - Its vasoconstrictive properties make it useful topically to reduce **bleeding** during and after surgical procedures like **adenoidectomy**. *Rhino cerebral mucormycosis* - This is a serious fungal infection requiring systemic antifungal therapy, often **amphotericin B**. Topical phenylephrine has no role in treating the infection itself. - While bleeding might be a symptom of mucormycosis, phenylephrine would only offer temporary symptomatic relief, not address the underlying fungal pathology. *Inlay type I myringoplasty* - Myringoplasty is a surgical procedure to repair a perforated eardrum. Topical phenylephrine is not indicated for this procedure. - The primary goal of this surgery is to reconstruct the **tympanic membrane**, and phenylephrine would not contribute to tissue healing or graft integration. *Subglottic stenosis* - This condition involves narrowing of the airway below the vocal cords, often requiring surgical intervention or corticosteroids. - Phenylephrine is a decongestant and vasoconstrictor, and as such, it does not have a therapeutic role in resolving the **fibrotic narrowing** characteristic of subglottic stenosis.
Question 3: A child who underwent a tonsillectomy started bleeding while lying in the ward post-operatively. Which of the following is the most appropriate management step?
- A. Take to OT, remove the clot & re-ligation (Correct Answer)
- B. Conservative management
- C. Take to OT & pressure packing
- D. Cautery
Explanation: ***Take to OT, remove the clot & re-ligation*** - **Post-tonsillectomy bleeding** is a surgical emergency requiring immediate intervention to prevent airway compromise and significant blood loss. - The most definitive management involves returning to the **operating theatre** for direct visualization, removal of any obstructing clots, and **re-ligation** of the bleeding vessel. *Conservative management* - **Conservative management** is generally insufficient for significant post-tonsillectomy bleeding, as it does not address the source of hemorrhage and can lead to severe complications. - While minor oozing might be observed, active bleeding often indicates a larger vessel injury that requires **surgical hemostasis**. *Take to OT & pressure packing* - While **pressure packing** can temporarily slow bleeding, it is not a definitive long-term solution as it does not directly identify and treat the bleeding vessel. - Furthermore, pharyngeal packing in a child carries a risk of **airway obstruction** and aspiration, making it less suitable than direct re-ligation. *Cautery* - **Cautery** is a method of hemostasis, but it is typically performed in the operating theatre under direct vision, often after clot removal. - It is not a stand-alone initial management step in the ward for active bleeding without proper surgical assessment and preparation.
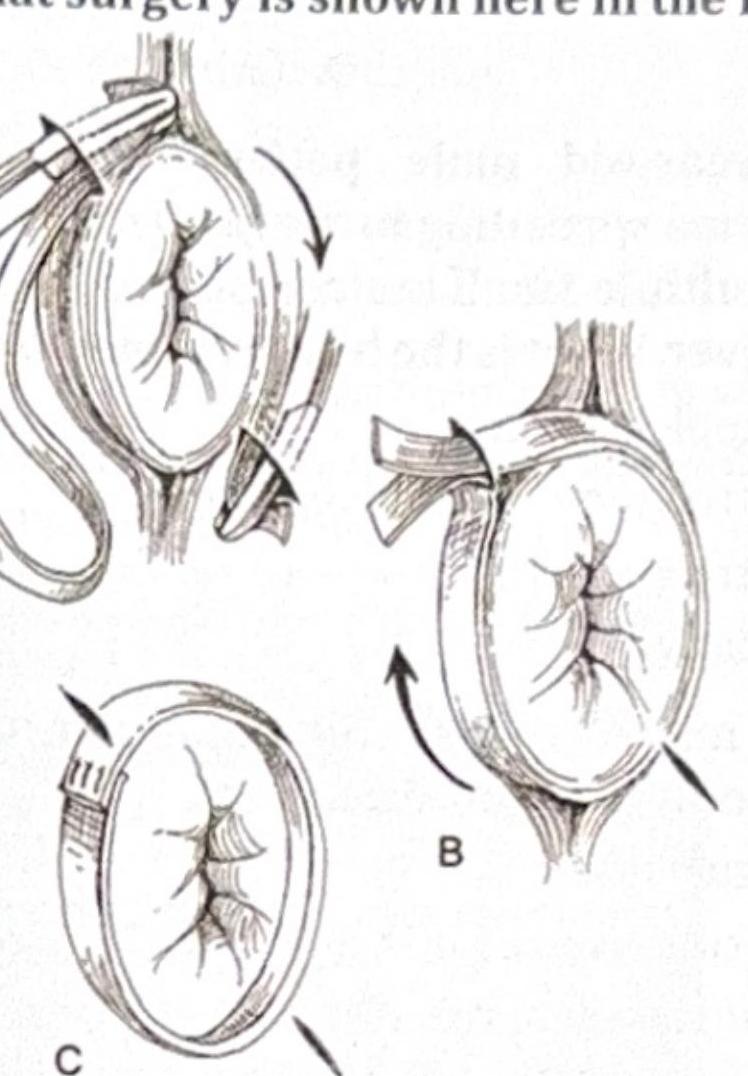
Question 4: What surgery is shown here in the image?
- A. Hemorrhoidectomy
- B. Altemeier operation
- C. Wells procedure
- D. Thiersch wiring (Correct Answer)
Explanation: ***Thiersch wiring*** - The image clearly depicts a **suture or wire** placed circumferentially around the anus to reduce its caliber, which is the hallmark of a **Thiersch procedure**. - This technique is used to treat **anal incontinence** by constricting the anal opening and improving sphincter function. *Hemorrhoidectomy* - This procedure involves the **surgical removal of hemorrhoids** and the images do not show any identifiable hemorrhoidal tissue being excised. - While bleeding and prolapse can be associated with hemorrhoids, the depicted technique with circumferential wiring is not used for their removal. *Altemeier operation* - The Altemeier operation is a type of **perineal rectosigmoidectomy** for rectal prolapse that involves resecting the prolapsed segment of the rectum. - The image does not illustrate resection of rectal tissue; instead, it shows a constricting device around the anus. *Wells procedure* - The Wells procedure, or **rectopexy**, involves anchoring the rectum to the sacrum to correct rectal prolapse. - This procedure typically involves an abdominal approach and fixation techniques, which are not represented in the illustration.
Question 5: A patient presents with upper limb swelling after undergoing a modified radical mastectomy (MRM). What is the most likely cause?
- A. Angiosarcoma
- B. Recurrence
- C. Upper limb Lymphedema (Correct Answer)
- D. Metastasis
Explanation: ***Upper limb Lymphedema*** - **Lymphedema** is a common complication after **modified radical mastectomy (MRM)** due to the removal of axillary lymph nodes and subsequent disruption of lymphatic drainage pathways. - This disruption leads to an accumulation of lymphatic fluid in the interstitial tissues, causing **swelling** in the ipsilateral upper limb. *Angiosarcoma* - **Angiosarcoma** (Stewart-Treves syndrome) is a very rare, aggressive tumor that can occur in the chronic lymphedematous limb after mastectomy. - It presents as multiple **violaceous nodules or plaques** in the affected limb, which is not described as the initial finding. *Recurrence* - **Recurrence** of breast cancer in the axilla or chest wall could cause swelling, but it would typically involve a palpable mass, skin changes, or pain, which are not mentioned as the primary symptom. - While recurrence can lead to lymphatic obstruction, **lymphedema** is a more direct and common post-operative complication. *Metastasis* - **Metastasis** to the axillary or supraclavicular lymph nodes could cause lymphatic obstruction and swelling. - However, lymphedema from direct surgical disruption of lymphatics is a more immediate and common cause of upper limb swelling following MRM, especially without other signs of widespread disease.
Question 6: Which of the following is the most commonly performed repair for a direct inguinal hernia?
- A. Lichtenstein repair (Correct Answer)
- B. Bassini's repair
- C. Herniotomy
- D. All of the options
Explanation: ***Lichtenstein repair*** - The **Lichtenstein repair** is a **tension-free mesh repair** and is the most commonly performed technique for direct inguinal hernias due to its low recurrence rates. - This technique involves placing a **synthetic mesh** over the deficient posterior wall of the inguinal canal, reinforcing the weakened area. *Bassini's repair* - **Bassini's repair** is a tissue-based repair that involves suturing the conjoined tendon to the inguinal ligament. - It creates tension on the repair, which historically led to **higher recurrence rates** compared to mesh repairs. *Herniotomy* - **Herniotomy** is the surgical removal of the **hernia sac** without repairing the defect in the abdominal wall. - This procedure is typically reserved for **pediatric patients** with indirect inguinal hernias due to the good intrinsic muscle tone and relatively small defect, but it is not the primary repair for direct inguinal hernias in adults. *All of the options* - While all listed procedures are methods for hernia management, only the **Lichtenstein repair** is considered the most commonly performed repair for direct inguinal hernias in current practice. - The other options are less commonly performed or reserved for specific patient populations.
Question 7: A patient presents with breathlessness and decreased air entry into the right lung following a road traffic accident (RTA) and is hypotensive. What is the next step in management?
- A. Wide bore needle decompression
- B. Needle insertion at 5th ICS in mid-axillary line
- C. Needle insertion at 2nd ICS in midclavicular line (MCL) (Correct Answer)
- D. Fluid resuscitation using wide bore cannula
Explanation: ***Needle insertion at 2nd ICS in midclavicular line (MCL)*** - The combination of **breathlessness**, **decreased air entry**, **hypotension** following trauma indicates a **tension pneumothorax**, which requires immediate decompression. - **Needle decompression** at the **2nd intercostal space (ICS)** in the **midclavicular line (MCL)** is the recommended immediate life-saving procedure to relieve pressure according to **ATLS guidelines**. - This option is the **most complete and precise answer**, specifying both the procedure and the exact anatomical location needed for safe execution. *Wide bore needle decompression* - While this correctly identifies the procedure type (needle decompression with a wide bore needle), it lacks the **critical anatomical specification** needed for clinical application. - In an emergency, knowing **where** to insert the needle is as important as knowing to perform the procedure - **2nd ICS at MCL** is the standard taught location. - This option is incomplete compared to the option that specifies the exact anatomical landmark. *Needle insertion at 5th ICS in mid-axillary line* - The **5th ICS in the mid-axillary line** is the appropriate location for inserting a **chest drain (tube thoracostomy)**, which is a definitive treatment but not the immediate emergency intervention. - For **tension pneumothorax**, immediate **needle decompression at 2nd ICS MCL** must be performed first to relieve life-threatening pressure, followed by chest tube insertion. - Using this location for initial needle decompression is not standard ATLS protocol. *Fluid resuscitation using wide bore cannula* - While **fluid resuscitation** is important for a trauma patient with hypotension, it will not address the primary life-threatening issue of **tension pneumothorax**. - The immediate priority is to relieve the pressure on the heart and lungs, as hypotension in this context is due to **obstructive shock** from impaired venous return and cardiac output. - Fluids alone will not correct the mechanical obstruction caused by the tension pneumothorax.
Question 8: After a total thyroidectomy, the surgeon is unable to extubate the patient, who shows cyanosis and respiratory distress. What is the most likely cause of the inability to extubate?
- A. Bilateral recurrent laryngeal nerve palsy (Correct Answer)
- B. Unilateral recurrent laryngeal nerve palsy
- C. Superior laryngeal nerve palsy
- D. Hemorrhage
Explanation: ***Bilateral recurrent laryngeal nerve palsy*** - After total thyroidectomy, injury to both **recurrent laryngeal nerves** can lead to paralysis of the abductor muscles of the vocal cords causing them to approximate, leading to **airway obstruction**, cyanosis, and respiratory distress. - This condition prevents successful extubation and often necessitates **reintubation** or **tracheostomy**. *Unilateral recurrent laryngeal nerve palsy* - Causes **hoarseness** due to unilateral vocal cord paralysis but typically does not result in severe airway obstruction or inability to extubate. - The unaffected vocal cord can usually compensate sufficiently to maintain an adequate airway for breathing. *Superior laryngeal nerve palsy* - Primarily affects the **protective reflexes of the larynx** and vocal cord tension (pitch), leading to issues like **aspiration risk** and a weak, breathy voice. - It does not directly cause vocal cord paralysis in a position that obstructs the airway. *Hemorrhage* - While a significant **post-operative hemorrhage** in the neck can cause airway compression and respiratory distress, it usually manifests as **neck swelling** and possibly hypovolemic shock. - The scenario explicitly states "inability to extubate," suggesting a vocal cord issue rather than external compression by a hematoma.
Question 9: Asymptomatic varicose veins would fall under which category of the CEAP classification system?
- A. C1 (Telangiectasias or reticular veins)
- B. C2 (Varicose veins) (Correct Answer)
- C. C3 (Edema)
- D. C4 (Skin changes)
Explanation: ***C2 (Varicose veins)*** - The CEAP classification uses 'C' for clinical manifestations, with **C2 specifically indicating the presence of varicose veins**. - Since the patient has **asymptomatic varicose veins**, C2 accurately captures this clinical state without implying more severe complications. - Varicose veins are classified as C2 **regardless of whether they are symptomatic or asymptomatic**. *C1 (Telangiectasias or reticular veins)* - C1 refers to smaller veins, such as **telangiectasias (spider veins)** and **reticular veins**, which are distinct from the larger, tortuous varicose veins. - These are less prominent venous abnormalities compared to varicose veins. *C3 (Edema)* - C3 indicates the **presence of edema** due to venous insufficiency. - The question specifies **asymptomatic varicose veins** without mention of edema, making C3 incorrect. *C4 (Skin changes)* - C4 denotes **skin changes** related to chronic venous insufficiency, such as pigmentation, eczema, or lipodermatosclerosis. - These are more advanced signs of venous disease and are not present in a patient with only varicose veins without complications.
Question 10: Which nerve is most commonly injured during submandibular gland surgery?
- A. Lingual nerve
- B. Marginal mandibular branch of facial nerve (Correct Answer)
- C. Mylohyoid nerve
- D. Hypoglossal nerve
Explanation: ***Marginal mandibular branch of facial nerve*** - The **marginal mandibular nerve** courses superficially over and along the superior border of the submandibular gland, making it the **most vulnerable** structure during surgery - It is at highest risk during elevation of the gland, ligation of the facial vessels, and dissection near the gland's superior border - Injury leads to **weakness or paralysis of the depressor muscles of the lower lip** (depressor anguli oris and depressor labii inferioris), causing an asymmetric smile and difficulty with lip movements - This is the **most common nerve injury** in submandibular gland surgery due to its superficial anatomical position *Incorrect: Lingual nerve* - The **lingual nerve** passes medial to the submandibular duct and deep to the gland - While it can be injured during dissection of the submandibular duct or deeper aspects of the gland, it is **less commonly injured** than the marginal mandibular nerve - Damage results in **loss of taste and general sensation** to the anterior two-thirds of the tongue on the ipsilateral side *Incorrect: Mylohyoid nerve* - The **mylohyoid nerve** travels on the inferior surface of the mylohyoid muscle, generally beneath and protected by this muscle - It supplies the mylohyoid and anterior belly of the digastric muscles - Injury is **uncommon** during routine submandibular gland excision due to its protected anatomical position *Incorrect: Hypoglossal nerve* - The **hypoglossal nerve** lies deep and inferior to the submandibular gland - It supplies motor innervation to the intrinsic and extrinsic muscles of the tongue - It is the **least commonly injured** nerve as it is well-protected by its deep position, unless dissection is carried excessively deep or inferiorly