All (182)Anatomy (10)Anatomy (1)Anesthesiology (3)Behavioral Science (1)Biochemistry (8)Biochemistry (1)Biostatistics (1)Community Medicine (8)Dermatology (4)ENT (4)General Medicine (1)Internal Medicine (14)Internal Medicine (10)Management (1)Microbiology (14)OB/GYN (11)Obstetrics and Gynecology (11)Ophthalmology (8)Orthopaedics (3)Pathology (6)Patient Safety (3)Pediatrics (1)Pediatrics (14)Pharmacology (18)Pharmacology (1)Physiology (6)Radiology (4)Surgery (15)
Q51
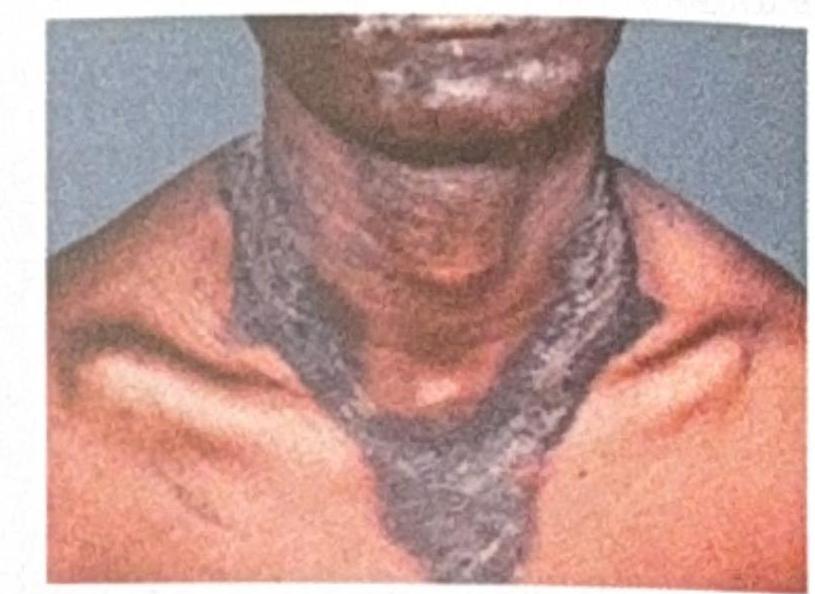
A 45-year-old man presents with the following skin changes (as shown in the image). What relevant history should be taken to diagnose this condition?