All (182)Anatomy (10)Anatomy (1)Anesthesiology (3)Behavioral Science (1)Biochemistry (8)Biochemistry (1)Biostatistics (1)Community Medicine (8)Dermatology (4)ENT (4)General Medicine (1)Internal Medicine (14)Internal Medicine (10)Management (1)Microbiology (14)OB/GYN (11)Obstetrics and Gynecology (11)Ophthalmology (8)Orthopaedics (3)Pathology (6)Patient Safety (3)Pediatrics (1)Pediatrics (14)Pharmacology (18)Pharmacology (1)Physiology (6)Radiology (4)Surgery (15)
Q131
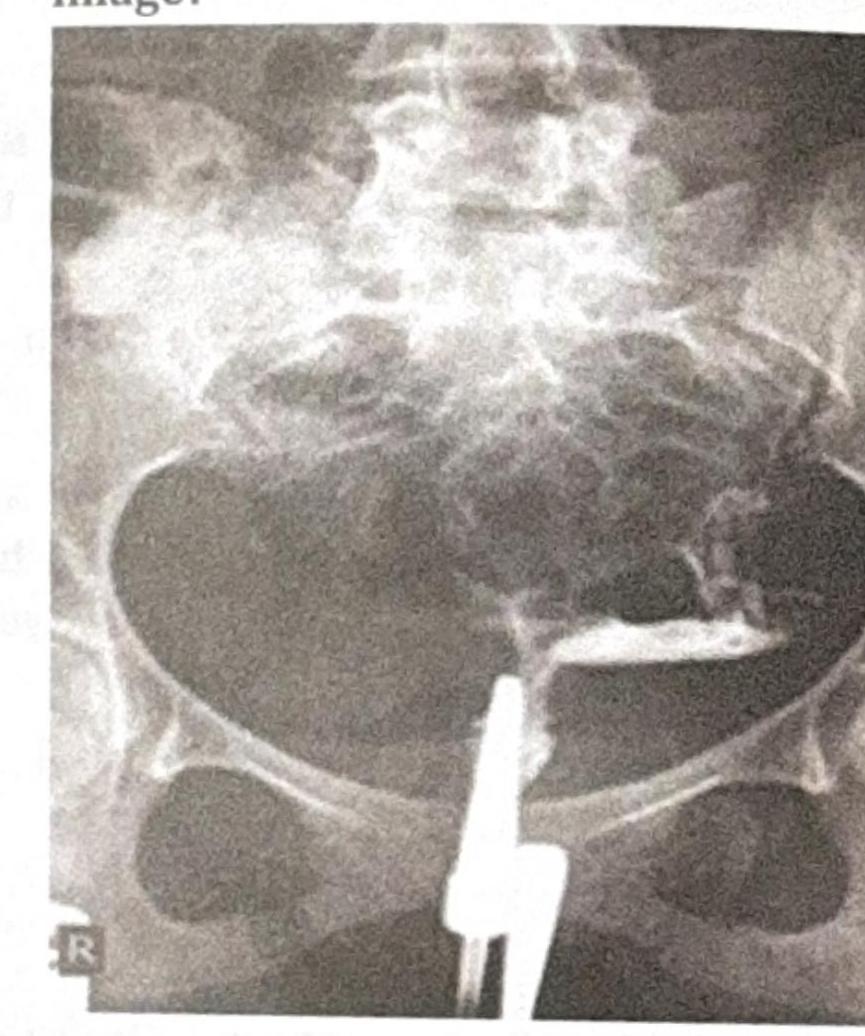
A 26-year-old male presents with backache, morning stiffness, reduced chest expansion, and reddening of the eyes. The X-ray provided is shown below. What is the most likely diagnosis?
Q132
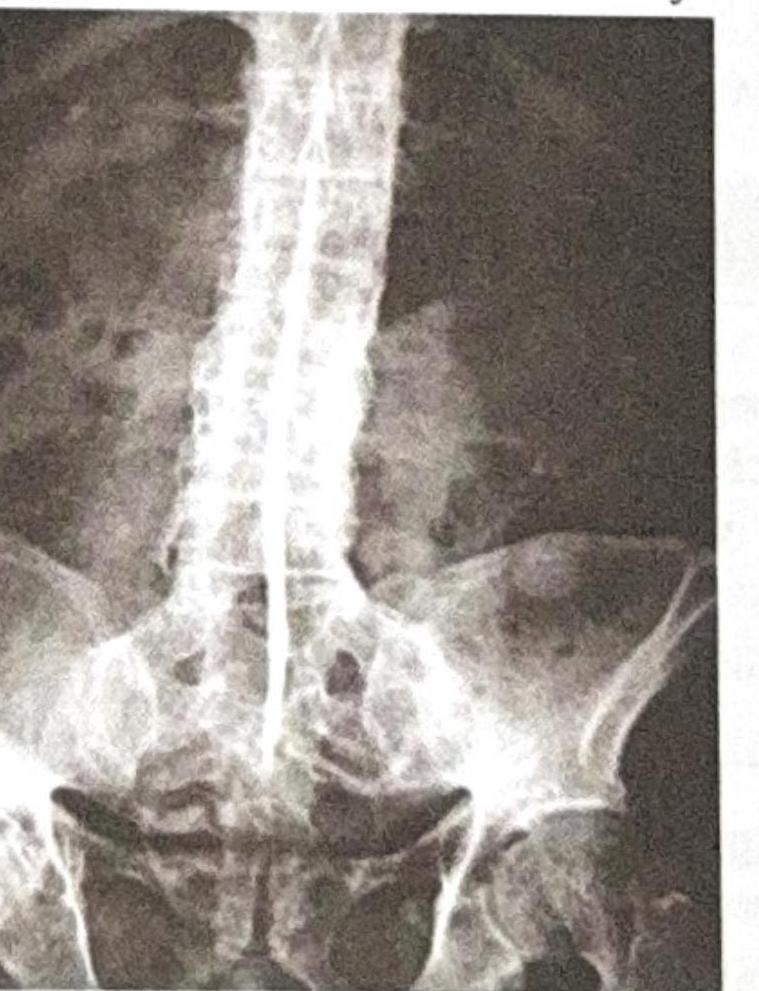
A 20-year-old patient presents with chronic low backache and early morning stiffness for the last 2 years. For the past 6 months, they have also experienced bilateral heel pain. What is the most likely diagnosis?