All (182)Anatomy (10)Anatomy (1)Anesthesiology (3)Behavioral Science (1)Biochemistry (8)Biochemistry (1)Biostatistics (1)Community Medicine (8)Dermatology (4)ENT (4)General Medicine (1)Internal Medicine (14)Internal Medicine (10)Management (1)Microbiology (14)OB/GYN (11)Obstetrics and Gynecology (11)Ophthalmology (8)Orthopaedics (3)Pathology (6)Patient Safety (3)Pediatrics (1)Pediatrics (14)Pharmacology (18)Pharmacology (1)Physiology (6)Radiology (4)Surgery (15)
Q121
What is the characteristic metabolic finding in a baby with Congenital Hypertrophic Pyloric Stenosis (CHPS)?
Q122
A child presents with rachitic changes in the limbs that are not responding to Vitamin D supplementation. Investigations reveal the following results: - Calcium: $9.5 \mathrm{mg} / \mathrm{dl}$ - Phosphorus: $1.6 \mathrm{mg} / \mathrm{dl}$ - Alkaline phosphatase (ALP): 814 IU - Serum PTH: $24.2 \mathrm{pg} / \mathrm{ml}$ - Serum electrolytes, creatinine, and blood gases: Normal. What is the most likely diagnosis?
Q123
Which vaccine is contraindicated in a 3-monthold infant with recurrent respiratory illness?
Q124
In a child with a height-for-age Z-score of less than -2 standard deviations (SD), what is the most likely cause?
Q125
A child presents with myoclonic jerks and decreasing school performance. The child had a history of fever and rash at the age of 1 year. What is the most likely diagnosis?
Q126
A child presents with a webbed neck, short stature, and a low posterior hairline. What is the most likely diagnosis?
Q127
A 10-year-old male presents with generalized edema. His cholesterol level is $238 \mathrm{mg} / \mathrm{dl}$, urine protein is $3+$, and stool microscopy shows fat in the stool. What is the most likely diagnosis?
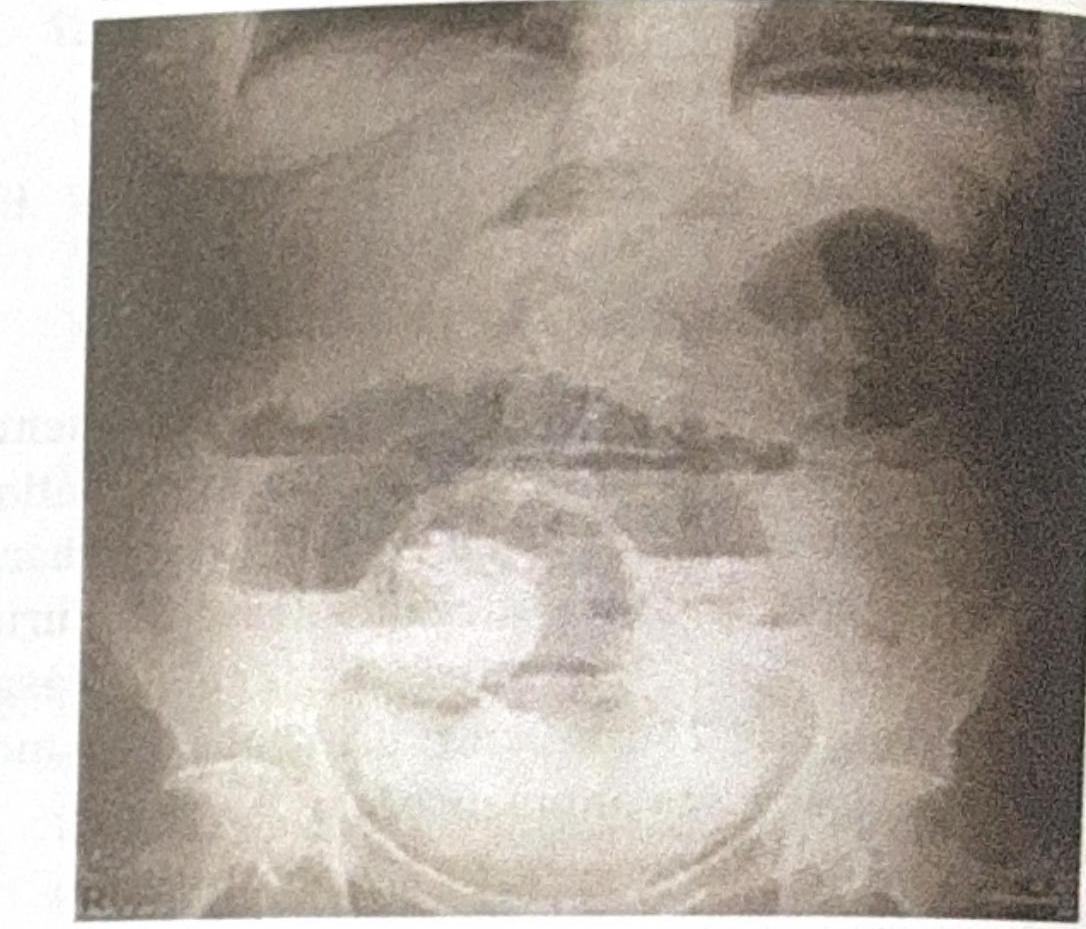
Q128
An X-ray of a 5-year-old child is shown below. The bone mineral density is normal. What is the most likely diagnosis?