All (182)Anatomy (10)Anatomy (1)Anesthesiology (3)Behavioral Science (1)Biochemistry (8)Biochemistry (1)Biostatistics (1)Community Medicine (8)Dermatology (4)ENT (4)General Medicine (1)Internal Medicine (14)Internal Medicine (10)Management (1)Microbiology (14)OB/GYN (11)Obstetrics and Gynecology (11)Ophthalmology (8)Orthopaedics (3)Pathology (6)Patient Safety (3)Pediatrics (1)Pediatrics (14)Pharmacology (18)Pharmacology (1)Physiology (6)Radiology (4)Surgery (15)
Q101
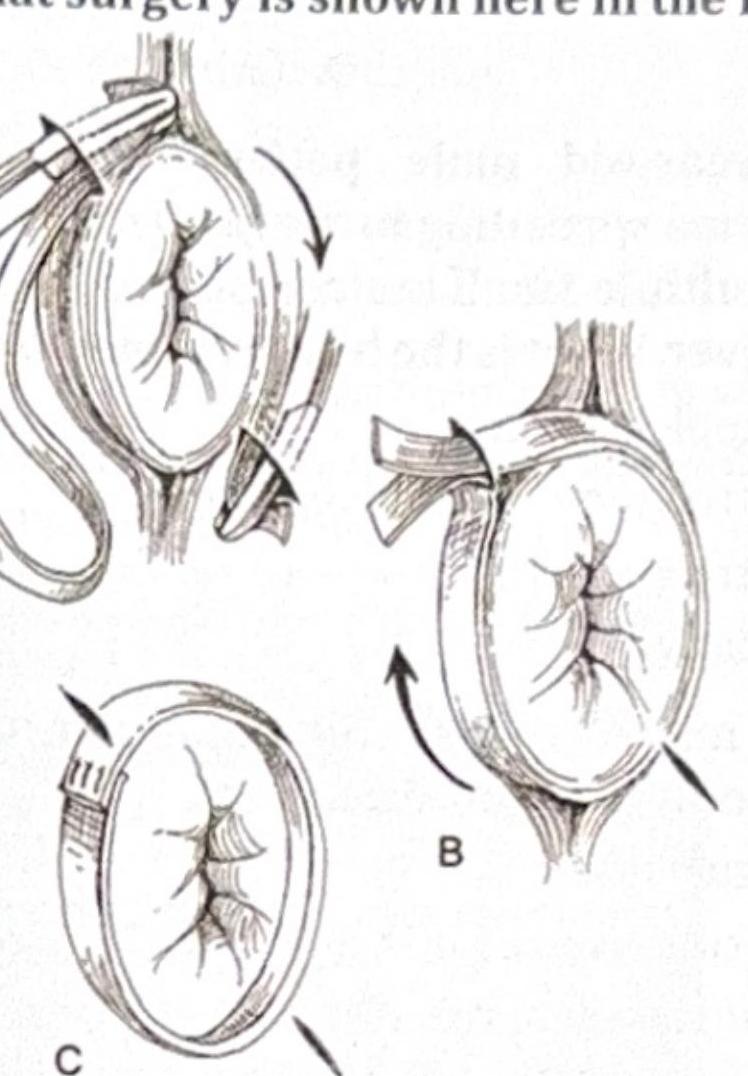
What surgery is shown here in the image?
Q102
A patient presents with upper limb swelling after undergoing a modified radical mastectomy (MRM). What is the most likely cause?
Q103
Which of the following is the most commonly performed repair for a direct inguinal hernia?
Q104
A patient presents with breathlessness and decreased air entry into the right lung following a road traffic accident (RTA) and is hypotensive. What is the next step in management?