All (182)Anatomy (10)Anatomy (1)Anesthesiology (3)Behavioral Science (1)Biochemistry (8)Biochemistry (1)Biostatistics (1)Community Medicine (8)Dermatology (4)ENT (4)General Medicine (1)Internal Medicine (14)Internal Medicine (10)Management (1)Microbiology (14)OB/GYN (11)Obstetrics and Gynecology (11)Ophthalmology (8)Orthopaedics (3)Pathology (6)Patient Safety (3)Pediatrics (1)Pediatrics (14)Pharmacology (18)Pharmacology (1)Physiology (6)Radiology (4)Surgery (15)
Q91
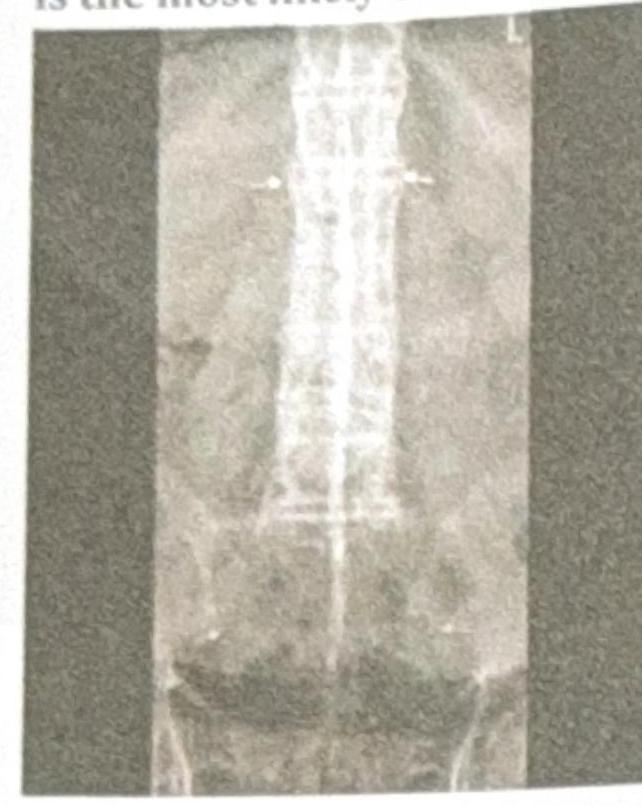
A young male presents with acute redness of the eye. His X-ray of the spine is shown below. What is the most likely condition?
Q92
A 56-year-old patient developed excruciating chest discomfort in the past 72 hours, relieved by GTN spray. Troponin I is normal, and the ECG shows features of left ventricular hypertrophy (LVH) with T wave flattening. The patient is already on statins, aspirin, and metoprolol 50 mg . What is the next best step in management?
Q93
A patient presents with a mediastinal mass and is diagnosed with pure red cell aplasia. What is the most probable underlying cause?
Q94
A 68-year-old male presents with cough, sputum production, bronchial breath sounds, respiratory rate of 20/min, urea of 44 mg/dl, and BP of 110/70 mmHg. What is the next step in management?
Q95
A patient presents with numb fingertips and tight facial skin. ANA is positive with an immunofluorescence nucleolar pattern. What is the most likely diagnosis?