A 30-year-old woman presents with flaccid bullae on her skin that are easy to rupture. A biopsy of the lesion reveals a suprabasal split. What is the most likely diagnosis?
Q2
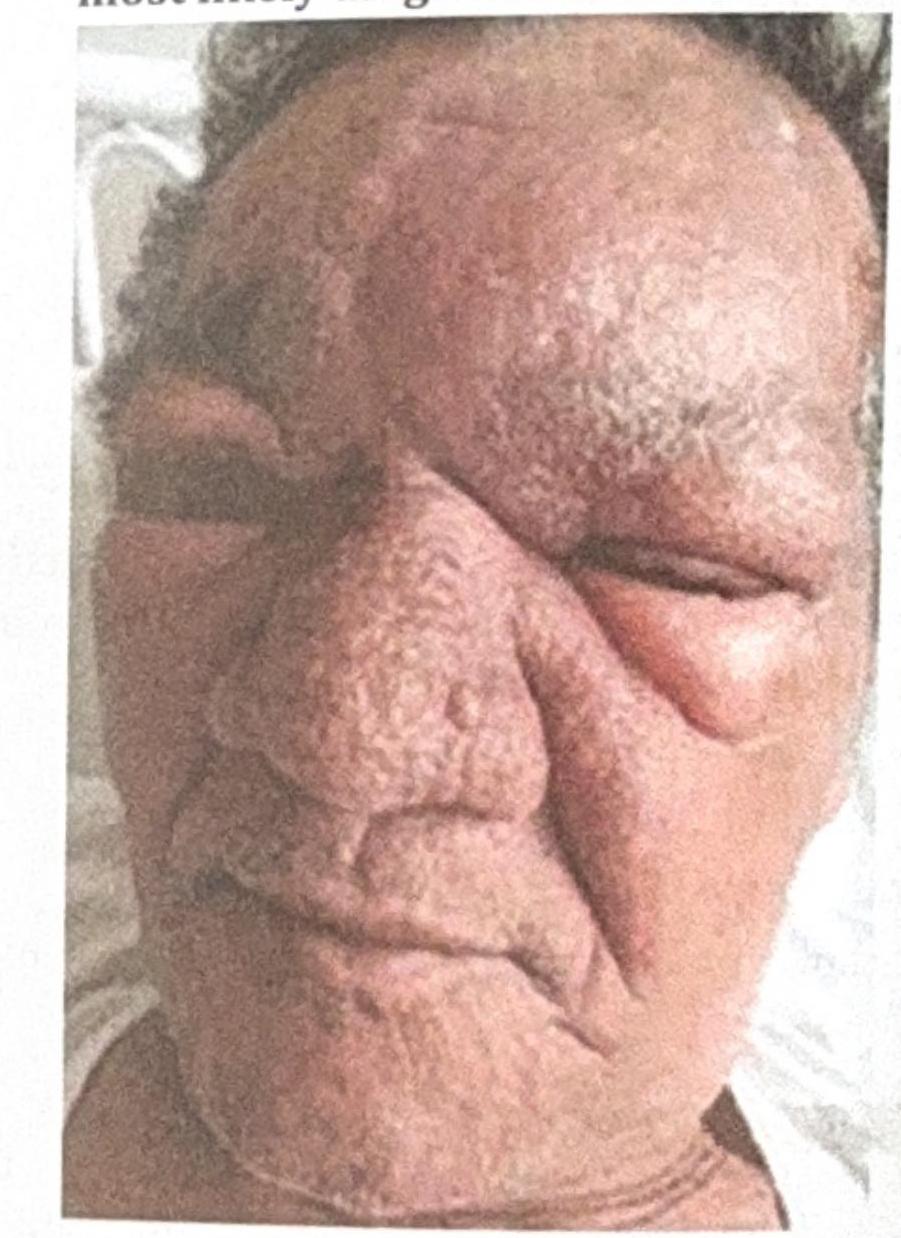
A 53 year-old male presented with erythematous, edematous plaques on his face over pre-existing hypoesthetic patches. He has been experiencing pain for the last 10 days and has been on multibacillary multidrug therapy (MBMDT) for leprosy for the past two months. What is the most likely diagnosis based on the image?
Q3
A young girl presents to the outpatient department with rough-surfaced lesions over her elbows and knees. She also complains of diminished vision at night. What is the most likely diagnosis?
NEET-PG 2021 - Dermatology NEET-PG Practice Questions and MCQs
Question 1: A 30-year-old woman presents with flaccid bullae on her skin that are easy to rupture. A biopsy of the lesion reveals a suprabasal split. What is the most likely diagnosis?
A. Erythema multiforme
B. Pemphigus vegetans
C. Pemphigus vulgaris (Correct Answer)
D. Pemphigus foliaceous
Explanation: ***Pemphigus vulgaris***
- Characterized by **flaccid bullae** that are easily ruptured, and a classic histological finding of a **suprabasal split** in the epidermis, indicating acantholysis just above the basal layer.
- Mucosal involvement is common, and the positive **Nikolsky sign** (epidermal detachment with lateral pressure) is often present, which is typical for pemphigus vulgaris due to the superficial nature of the blistering.
- The combination of **flaccid bullae + suprabasal split** is pathognomonic for pemphigus vulgaris.
*Erythema multiforme*
- Typically presents with **targetoid lesions** (concentric rings of erythema) and is often associated with infections, particularly herpes simplex virus (HSV).
- Histologically, it shows **interface dermatitis** with vacuolar degeneration of basal cells and scattered necrotic keratinocytes, not a suprabasal split or acantholysis.
*Pemphigus vegetans*
- A rare variant of pemphigus vulgaris, it presents with **vegetating plaques** in intertriginous areas (axillae, groin), which are eroded but not primarily flaccid bullae covering wide areas.
- While it also involves a suprabasal split at the same level as pemphigus vulgaris, the clinical presentation of vegetating plaques rather than widespread flaccid bullae helps differentiate it.
*Pemphigus foliaceous*
- This autoimmune blistering disease features very **superficial bullae** that rupture so easily they typically present as erosions, crusts, and scaling rather than intact blisters.
- Histologically, it shows a **subcorneal or granular layer split** (more superficial than pemphigus vulgaris), not the deeper suprabasal split seen in this patient's biopsy.
- Mucosal involvement is **rare** in pemphigus foliaceous, unlike pemphigus vulgaris.
Question 2: A 53 year-old male presented with erythematous, edematous plaques on his face over pre-existing hypoesthetic patches. He has been experiencing pain for the last 10 days and has been on multibacillary multidrug therapy (MBMDT) for leprosy for the past two months. What is the most likely diagnosis based on the image?
A. Type 1 Lepra reaction (Correct Answer)
B. Erythema Nodosum Leprosum (ENL)
C. Cellulitis of the face
D. Erysipelas
Explanation: ***Type 1 Lepra reaction***
- The patient presents with **erythematous, edematous plaques on pre-existing hypoesthetic patches** on the face, along with pain and current treatment with **multibacillary multidrug therapy (MBMDT)**. This clinical picture is classic for a type 1 lepra reaction, which is a **delayed-type hypersensitivity reaction** to *Mycobacterium leprae* antigens, often seen during or after treatment.
- The image shows significant **facial edema** and **erythema**, particularly around the eyes and nose, consistent with the acute inflammation of a type 1 reaction affecting existing skin lesions and nerves, leading to pain.
*Erythema Nodosum Leprosum (ENL)*
- ENL is a **Type 2 lepra reaction**, characterized by the appearance of **painful, tender, erythematous nodules** over normal skin, often affecting the limbs and trunk, not typically pre-existing hypoesthetic patches.
- It is an **immune complex-mediated reaction** and usually presents more acutely with systemic symptoms like fever and malaise, along with the characteristic nodules, which are not primarily visible in the photograph as widespread edematous plaques.
*Cellulitis of the face*
- Cellulitis is a **bacterial infection** of the deep dermis and subcutaneous tissue, presenting as a **spreading, warm, red, tender area** with poorly defined borders, often associated with fever and lymphadenopathy.
- While there is erythema and edema, the chronic nature of the underlying hypoesthetic patches, the patient's history of leprosy, and the specific distribution suggest a reaction related to leprosy rather than a typical acute bacterial infection.
*Erysipelas*
- Erysipelas is a **superficial bacterial skin infection**, typically caused by *Streptococcus pyogenes*, characterized by a **sharply demarcated, raised, red, warm, and tender plaque**, often on the face, with characteristic "peau d'orange" texture.
- Although it causes facial erythema and edema, the clearly defined borders of erysipelas are not evident, and the association with pre-existing hypoesthetic patches in a leprosy patient points more strongly towards a lepra reaction.
Question 3: A young girl presents to the outpatient department with rough-surfaced lesions over her elbows and knees. She also complains of diminished vision at night. What is the most likely diagnosis?
A. Folliculitis
B. Pyoderma
C. Keratosis pilaris
D. Phrynoderma (Correct Answer)
Explanation: ***Phrynoderma***
- Phrynoderma, also known as **follicular hyperkeratosis**, presents with **rough, horny papules** over extensor surfaces like elbows and knees, often described as "toad skin."
- It is a skin manifestation of **vitamin A deficiency**, which also causes **night blindness** (nyctalopia) due to impaired production of rhodopsin.
*Folliculitis*
- This is an **inflammation of hair follicles**, appearing as small, red bumps or pustules centered around hair follicles.
- It is typically caused by bacterial or fungal infections and does not cause **night blindness**.
*Pyoderma*
- **Pyoderma** refers to a **pus-producing skin infection** caused by bacteria, such as impetigo or cellulitis.
- These are characterized by crusts, blisters, or inflamed lesions and are not associated with **rough skin** or **night blindness**.
*Keratosis pilaris*
- This common genetic condition causes small, rough bumps, typically on the upper arms, thighs, and buttocks, due to **keratin plugging hair follicles**.
- While it causes rough skin similar to phrynoderma, it is generally **benign** and does not cause systemic symptoms like **night blindness**.