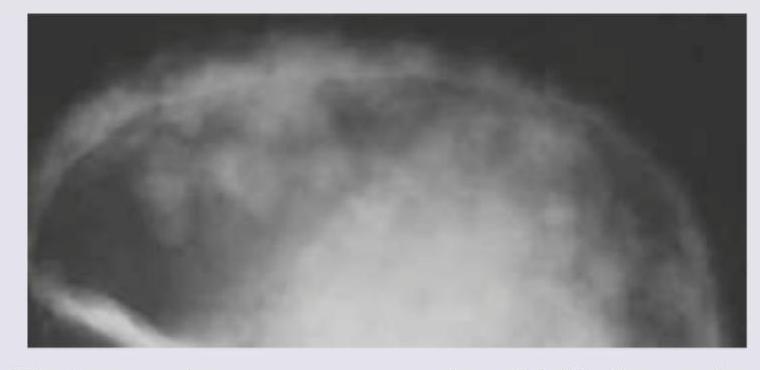
The following Skull X-ray is seen in:
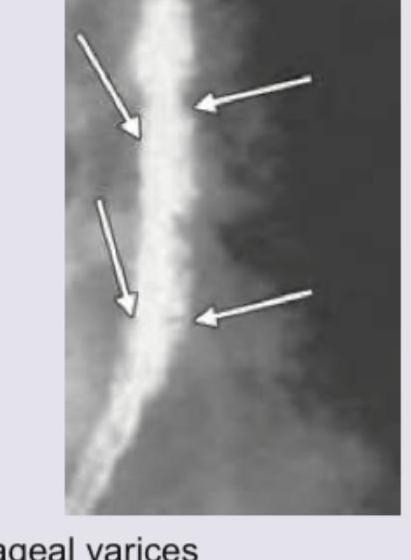
The following barium swallow study shows which of the following?
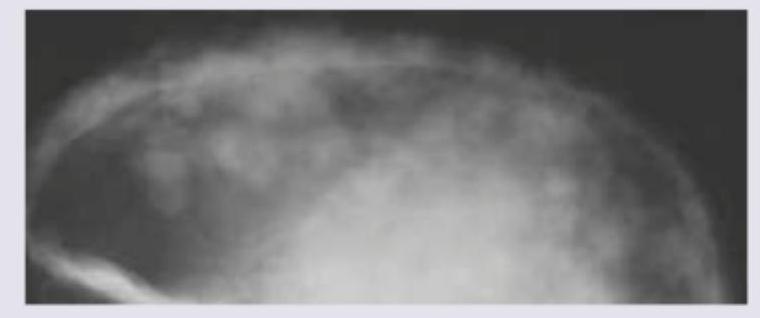
Which of the following will be the most probable diagnostic finding in the patient with X-Ray skull shown below?
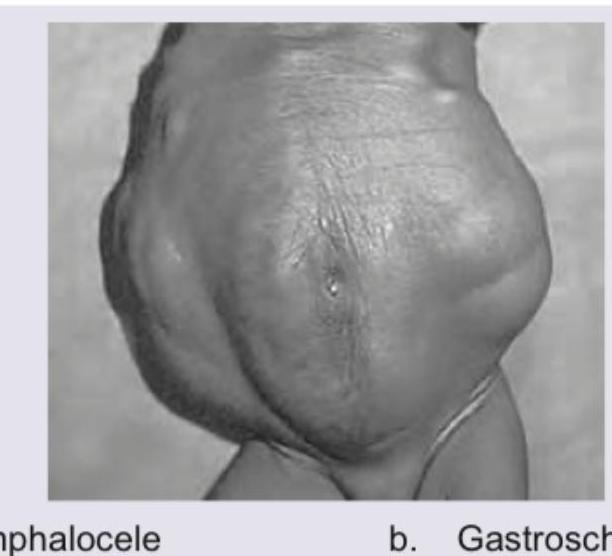
Identify this condition?
Identify the grade of vesico-ureteric reflux in the picture below?

The following test was performed on the patient. Which is correct about the patient?
The ultrasound finding of a 7 -month-old child with abdominal pain and mass in the upper abdomen is shown below. What is the diagnosis? (NEET Pattern 2018)
The following image shows the presence of?

The following X-ray is used to evaluate \qquad sinus?
A radiographic projection with X-ray beam angled at 30 degrees to the radiographic plate, with the skull positioned laterally (as shown in the image), is used to visualize which of the following structures?
NEET-PG 2018 - Radiology NEET-PG Practice Questions and MCQs
Question 21: The following Skull X-ray is seen in:
- A. Thalassemia (Correct Answer)
- B. Multiple myeloma
- C. Histiocytosis-X
- D. Paget's disease
Explanation: ***Thalassemia*** - The image shows a classic **hair-on-end appearance** of the skull, which is a characteristic radiological finding in severe forms of thalassemia. - This appearance results from **marrow hyperplasia** in response to chronic hemolysis, leading to widening of the diploic space and expansion of bone marrow at the expense of outer cortical bone. *Multiple myeloma* - Multiple myeloma typically presents with multiple well-demarcated, **punched-out lytic lesions** in the skull, without a "hair-on-end" pattern. - The bone lesions are due to plasma cell infiltration and osteoclast activation, leading to discrete areas of bone destruction. *Histiocytosis-X* - Histiocytosis-X, also known as Langerhans cell histiocytosis, can cause **lytic bone lesions** in the skull, often referred to as "geographic" or "punched-out" lesions. - While it can cause diffuse bone involvement, it does not typically produce the organized trabecular pattern characteristic of "hair-on-end." *Paget's disease* - Paget's disease of bone often manifests as areas of **bone enlargement**, cortical thickening, and a mixture of lytic and sclerotic changes, sometimes described as a **cotton-wool appearance** in the skull. - It does not present with the "hair-on-end" pattern, which is primarily associated with conditions causing chronic marrow expansion.
Question 22: The following barium swallow study shows which of the following?
- A. Esophageal varices (Correct Answer)
- B. Schatzki ring
- C. Candida esophagitis
- D. Reflux esophagitis
Explanation: ***Esophageal varices*** - The Barium Swallow image clearly demonstrates a **serpiginous**, worm-like, or **rosary bead-like appearance** along the esophageal wall, which is characteristic of esophageal varices. - Varices are dilated submucosal veins and appear as **filling defects** on barium studies, especially when distended. *Schatzki ring* - A Schatzki ring is a **thin, symmetric mucosal ring** at the esophagogastric junction, causing solid food dysphagia. - It presents as a **smooth, circumferential narrowing** on a barium swallow, which is not seen here. *Candida esophagitis* - Candida esophagitis typically appears as **ulcerations, plaques, or nodularity** with an irregular, cobblestone pattern on barium swallow. - This image does not show the characteristic **"shaggy" or "cobblestone"** appearance associated with candidal plaques. *Reflux esophagitis* - Reflux esophagitis can manifest as **mucosal irregularity, erosions, or strictures**, but not the distinct serpiginous filling defects seen in this image. - Severe reflux can cause peptic strictures, which appear as **smooth, tapered narrowings**, different from the irregular variceal pattern.
Question 23: Which of the following will be the most probable diagnostic finding in the patient with X-Ray skull shown below?
- A. Elevated SAP
- B. CD1A positivity (Correct Answer)
- C. Bence Jones proteins
- D. Elevated HbA2
Explanation: ***CD1A positivity*** - The skull X-ray shows multiple punched-out lytic lesions without sclerotic borders, characteristic of **Langerhans Cell Histiocytosis (LCH)**. - **Langerhans cells** in LCH express surface markers like **CD1a** and S100 protein, which are diagnostic when detected via **immunohistochemistry on tissue biopsy**. - CD1a positivity is the **gold standard** for confirming LCH diagnosis. *Elevated SAP* - **Serum Alkaline Phosphatase (SAP)** is typically elevated in conditions with increased osteoblastic activity or liver/biliary disease. - LCH lesions are generally **lytic** and not associated with increased osteoblastic activity, thus SAP elevation is not a specific or common finding. *Bence Jones proteins* - **Bence Jones proteins** (monoclonal light chains) are found in the urine of patients with **Multiple Myeloma**, which can also cause lytic bone lesions. - However, the image shows more discrete, "punched-out" lesions typical of LCH, whereas myeloma lesions are often more diffuse or "salt-and-pepper" in appearance, and LCH does not secrete Bence Jones proteins. *Elevated HbA2* - **Elevated HbA2** is a characteristic finding in **beta-thalassemia trait**, a genetic blood disorder. - There is no clinical or radiological indication in the provided image or question to suggest a connection to thalassemia.
Question 24: Identify this condition?
- A. Omphalocele
- B. Prune belly syndrome (Correct Answer)
- C. Gastroschisis
- D. Peritonitis
Explanation: ***Prune belly syndrome*** - The image shows the characteristic **wrinkled, prune-like appearance** of the abdominal wall due to **absent or deficient abdominal wall musculature**. - This condition is part of a triad including **urinary tract abnormalities** and **undescended testes** in males, with the distinctive loose, redundant abdominal skin. *Omphalocele* - An **omphalocele** presents with **abdominal contents herniating through the umbilical ring**, covered by a peritoneal membrane. - The image does not show any **herniated organs** or a sac-like protrusion at the umbilical area. *Gastroschisis* - **Gastroschisis** involves an **abdominal wall defect** typically to the right of the umbilical cord with **exposed bowel loops**. - No evidence of **herniated intestinal contents** or abdominal wall dehiscence is visible in this image. *Peritonitis* - **Peritonitis** is an **inflammatory condition** of the peritoneum presenting with abdominal rigidity and systemic signs. - This is not a structural abnormality visible externally but rather an **internal inflammatory process** requiring clinical assessment.
Question 25: Identify the grade of vesico-ureteric reflux in the picture below?
- A. Grade II
- B. Grade III
- C. Grade IV
- D. Grade V (Correct Answer)
Explanation: ***Grade V*** - This image shows **severe dilation** and **tortuosity of the ureter**, along with **blunting of the renal calyces** and loss of papillary impressions, extending all the way to the renal pelvis. - Grade V VUR indicates the most severe form of reflux, with significant distortion of the pelvicalyceal system, often associated with **renal parenchymal damage**. *Grade II* - Grade II VUR involves reflux into the **ureter, renal pelvis, and calyces**, but with **no dilation** and normal calyces. - The image clearly displays significant dilation and blunting of calyces, which is beyond Grade II. *Grade III* - In Grade III VUR, there is reflux into the **ureter** and **pelvicalyceal system (renal pelvis and calyces)** with **mild to moderate dilation** and slight blunting of the calyces. - The marked tortuosity and severe dilation seen in the image exceed the characteristics of Grade III. *Grade IV* - Grade IV VUR is characterized by **moderate to severe dilation** and **tortuosity of the ureter** and pelvicalyceal system, with **moderate blunting** of the calyces. - While there is severe dilation and tortuosity, the extent of calycial blunting and loss of papillary impressions in the image is more consistent with Grade V.
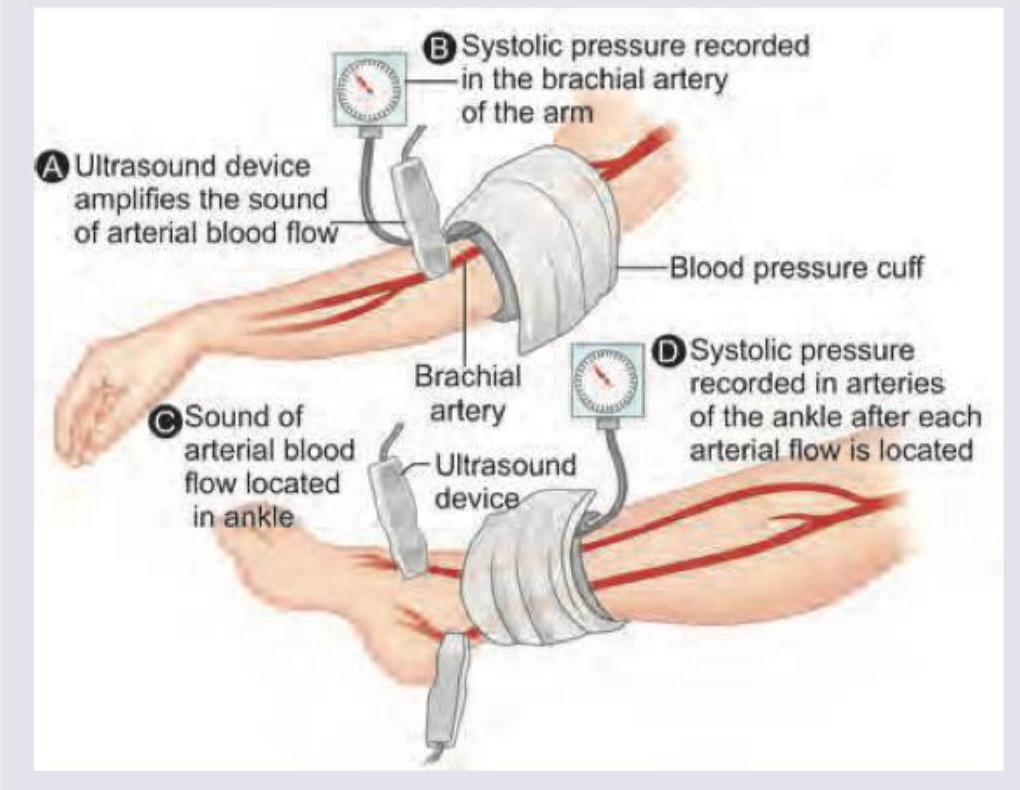
Question 26: The following test was performed on the patient. Which is correct about the patient?
- A. Pain is present at rest
- B. Pain decreases on standing still (Correct Answer)
- C. Pain is present on first step of walking
- D. Pain increases on limb dependency
Explanation: ***Pain decreases on standing still*** - The image depicts the measurement of **Ankle-Brachial Index (ABI)**, a diagnostic test for **Peripheral Artery Disease (PAD)**. - **Intermittent claudication** is the hallmark symptom of PAD, characterized by cramping pain in the legs that develops **after walking a certain distance** and is **relieved by rest** (standing still). - This occurs because the narrowed arteries cannot supply adequate blood flow during exercise, causing muscle ischemia and pain that resolves when activity ceases. *Pain is present on first step of walking* - This is **incorrect** for claudication, which requires time to develop as muscles become ischemic during sustained activity. - Pain on the **first step** would suggest **musculoskeletal pathology** (arthritis, plantar fasciitis) or **neurological issues** (nerve compression), not vascular claudication. - Claudication distance is a key diagnostic feature - patients can walk a reproducible distance before pain begins. *Pain is present at rest* - **Rest pain** indicates **critical limb ischemia**, a severe form of PAD where blood flow is inadequate even at rest. - This represents advanced arterial disease beyond simple claudication and requires urgent evaluation for revascularization. - Rest pain typically affects the forefoot and is worse at night when lying flat. *Pain increases on limb dependency* - Actually, **limb dependency (hanging the leg down)** typically **relieves pain** in severe PAD by using gravity to improve distal perfusion. - Patients with critical limb ischemia often sleep with legs dependent or dangle feet off the bed for relief. - This is opposite to **venous insufficiency**, where elevation improves symptoms.
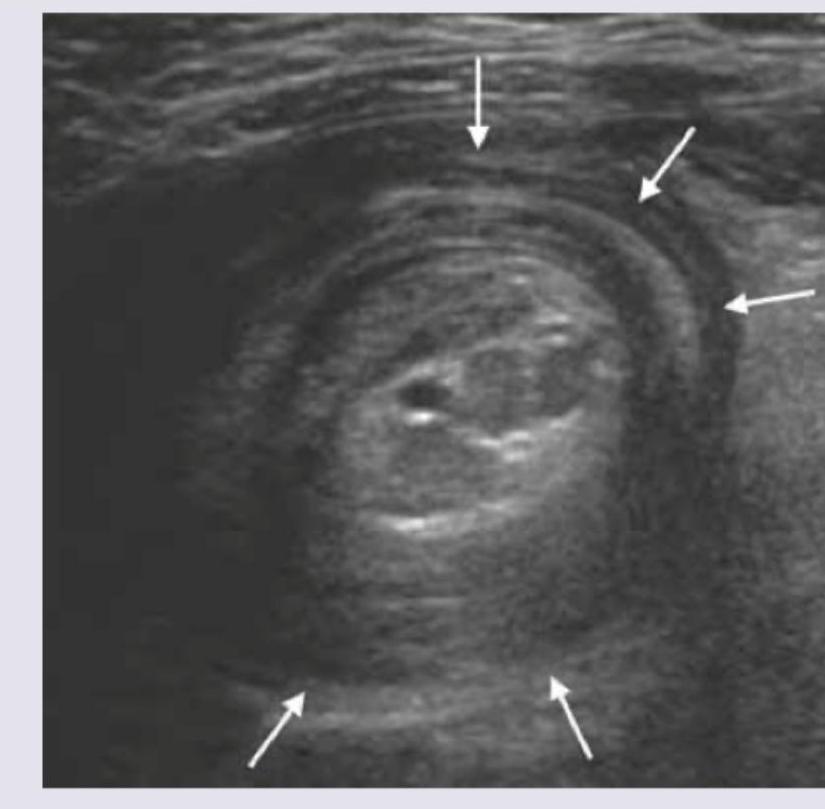
Question 27: The ultrasound finding of a 7 -month-old child with abdominal pain and mass in the upper abdomen is shown below. What is the diagnosis? (NEET Pattern 2018)
- A. Intestinal volvulus
- B. Intussusception (Correct Answer)
- C. Pyloric stenosis
- D. None of above
Explanation: ***Intussusception*** - The ultrasound image clearly shows a "target sign" or "doughnut sign," which is pathognomonic for **intussusception**, where one segment of the intestine telescopes into another. - This condition commonly presents in infants (around 6-36 months) with **abdominal pain**, an abdominal mass, and sometimes **currant jelly stools**. *Intestinal volvulus* - **Intestinal volvulus** involves the twisting of the intestine around its mesentery, which would typically show a "whirlpool sign" on ultrasound due to twisted mesenteric vessels, not the "target sign." - It usually presents with sudden onset of severe abdominal pain, bilious vomiting, and signs of intestinal obstruction and ischemia. *Pyloric stenosis* - **Pyloric stenosis** is characterized by hypertrophy of the pyloric muscle, which would appear as an elongated, thickened pyloric canal on ultrasound with increased pyloric muscle thickness (>3mm) and length (>15mm). - Clinical presentation involves non-bilious projectile vomiting in infants, typically between 2 and 8 weeks of age, not at 7 months with an abdominal mass and the bowel-within-bowel appearance shown. *None of above* - The classic ultrasound findings and clinical presentation strongly point to intussusception, making this option incorrect.
Question 28: The following image shows the presence of?
- A. Bladder stone (Correct Answer)
- B. Ureter stone
- C. Urethral stone
- D. Prostate calcification
Explanation: ***Bladder stone*** - The image displays multiple **radiopaque densities** (stones) clustered within the pelvic cavity, specifically in the region where the urinary bladder is anatomically located. - The aggregation and rounded shapes are characteristic of **vesical calculi** (bladder stones). *Ureter stone* - **Ureteral stones** would typically appear as a single or a few stones following the course of the ureters, which are tubular structures extending from the kidneys to the bladder. - The diffuse, multi-focal collection seen in the image is not consistent with the typical presentation of a ureteric calculus. *Urethral stone* - A **urethral stone** would be located within the urethra, which is inferior to the bladder and would typically present as a single, elongated calculus in the distal urinary tract. - The location and multiple, scattered appearance in the image do not match a urethral stone. *Prostate calcification* - **Prostatic calcifications** are usually smaller, often punctate, and concentrated within the confines of the prostatic gland, typically inferior to the bladder neck. - The calcifications in the image are larger and more widely distributed, not confined to the typical anatomical borders of the prostate.
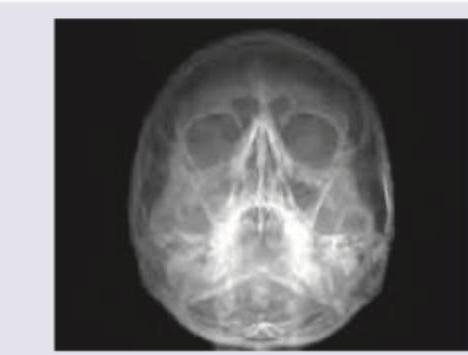
Question 29: The following X-ray is used to evaluate \qquad sinus?
- A. Frontal
- B. Maxillary (Correct Answer)
- C. Ethmoidal
- D. Sphenoidal
Explanation: ***Maxillary*** - The image provided is a **Waters' view** (occipitomental view) X-ray of the paranasal sinuses, which is primarily used to visualize the **maxillary sinuses**. - In a Waters' view, the **petrous ridges** (dense bone at the base of the skull) are projected below the maxillary sinuses, allowing for a clear view of these sinuses. *Frontal* - While the **frontal sinuses** are visible in a Waters' view, they are generally better visualized in a **Caldwell view** (occipitofrontal view) or lateral view. - In this projection, their visualization can be obscured by other bony structures, and they are not the primary focus. *Ethmoidal* - The **ethmoidal sinuses** are typically comprised of multiple small air cells located between the orbits and are best seen on a **Caldwell view** or specialized oblique views. - In a Waters' view, their evaluation is limited due to superimposition of other facial bones. *Sphenoidal* - The **sphenoidal sinuses** are located deep within the skull, inferior to the sella turcica, and are quite difficult to visualize on standard plain radiographs like the Waters' view. - They are best assessed using a **lateral view of the skull** or advanced imaging like **CT scans**.
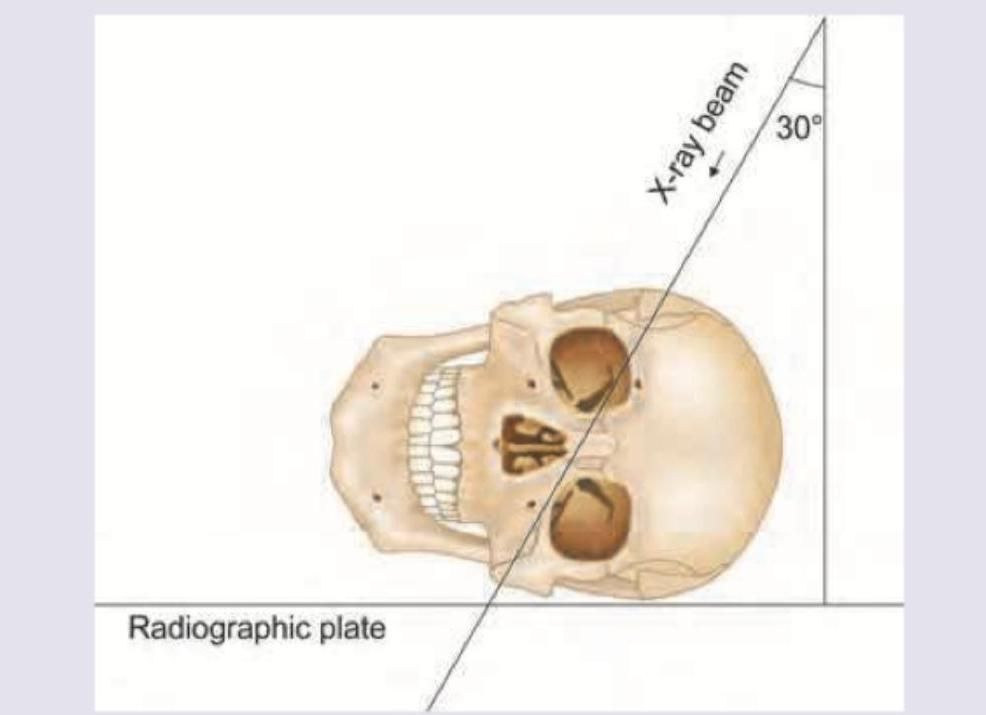
Question 30: A radiographic projection with X-ray beam angled at 30 degrees to the radiographic plate, with the skull positioned laterally (as shown in the image), is used to visualize which of the following structures?
- A. Sinus tympani (Correct Answer)
- B. Recess of fourth ventricle
- C. Round window
- D. Lateral ventricle
Explanation: ***Sinus tympani*** - The image shows a **radiographic projection** designed to visualize structures of the **temporal bone**. Specifically, an X-ray beam angled at 30 degrees to the radiographic plate, with the skull positioned laterally, is characteristic of specific views for the **middle ear structures**, such as the sinus tympani. - The **sinus tympani** is a small, deep recess in the posterior wall of the middle ear, and its detailed visualization often requires specialized **oblique radiographic projections**. *Recess of fourth ventricle* - The **fourth ventricle** is located within the brain stem, and its recesses are deep brain structures. - Visualization of the fourth ventricle and its recesses typically requires advanced imaging modalities like **CT or MRI**, not standard X-ray projections of the skull. *Round window* - The **round window** is a structure of the inner ear, specifically located at the cochlea. - While it is part of the temporal bone, standard skull X-rays are not optimal for its detailed visualization, and a specialized view for the **hypotympanum** would be needed to see it clearly, which is not depicted by this projection angle. *Lateral ventricle* - The **lateral ventricles** are located within the cerebral hemispheres of the brain. - Similar to the fourth ventricle, these structures are best visualized with **CT or MRI** and are not effectively seen with basic skull X-ray projections, especially not with an angled view designed for the temporal bone.