All SubjectsAnatomy (27)Anesthesiology (4)Biochemistry (28)Biochemistry (1)Community Medicine (12)Dental (1)Dermatology (8)ENT (4)Forensic Medicine (3)General Medicine (3)Internal Medicine (41)Microbiology (25)Obstetrics and Gynecology (24)Ophthalmology (3)Orthopaedics (6)Pathology (35)Pathology (4)Pediatrics (22)Pharmacology (23)Physiology (13)Psychiatry (8)Psychiatry (3)Radiology (26)Surgery (8)Surgery (34)
Q11
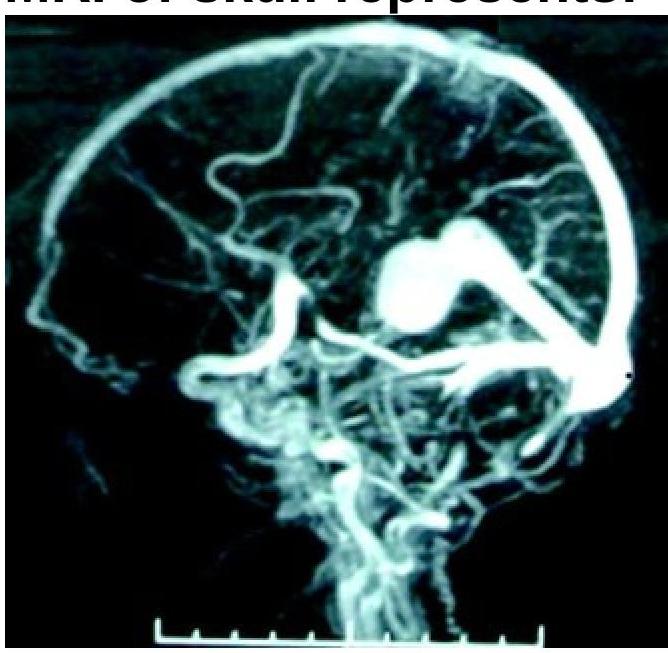
What condition is shown in the MR angiogram of the skull?
Q12
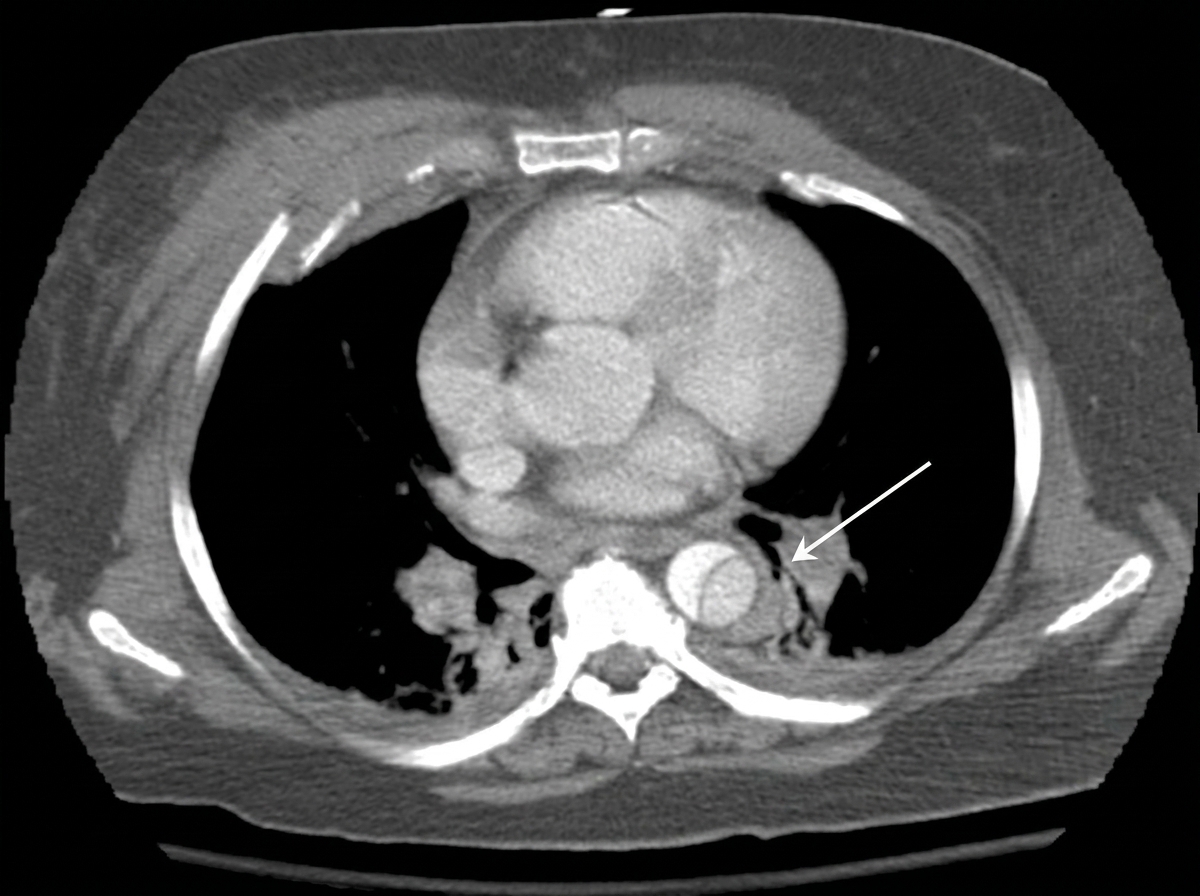
The CT thorax image shows:
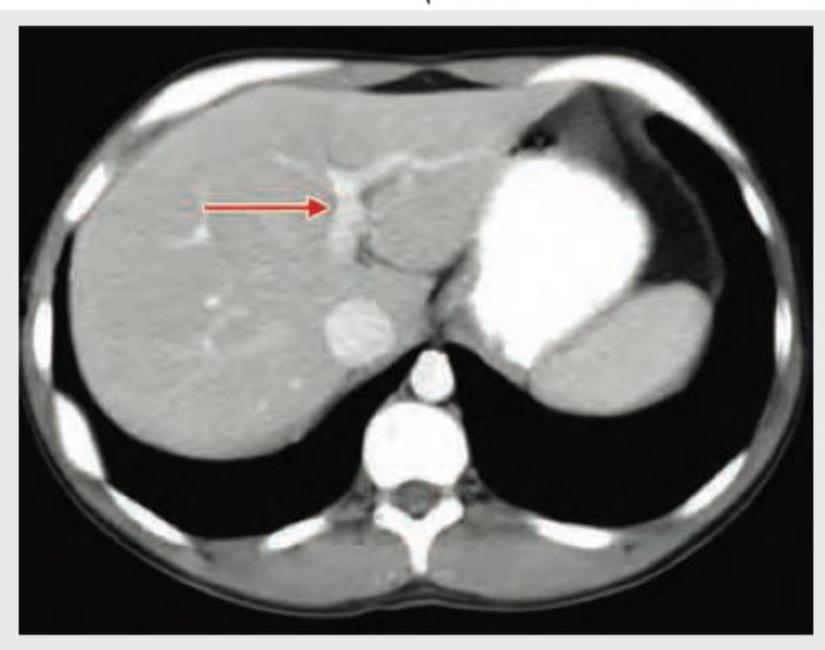
Q13
Identify the marked structure in the CT abdomen section shown below? (Recent NEET Pattern 2018-19)

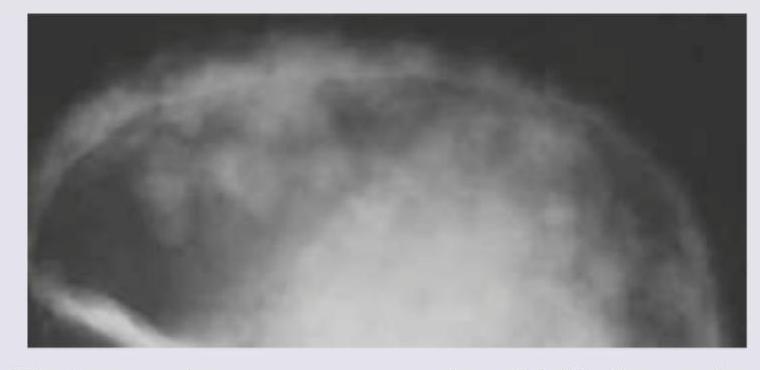
Q14
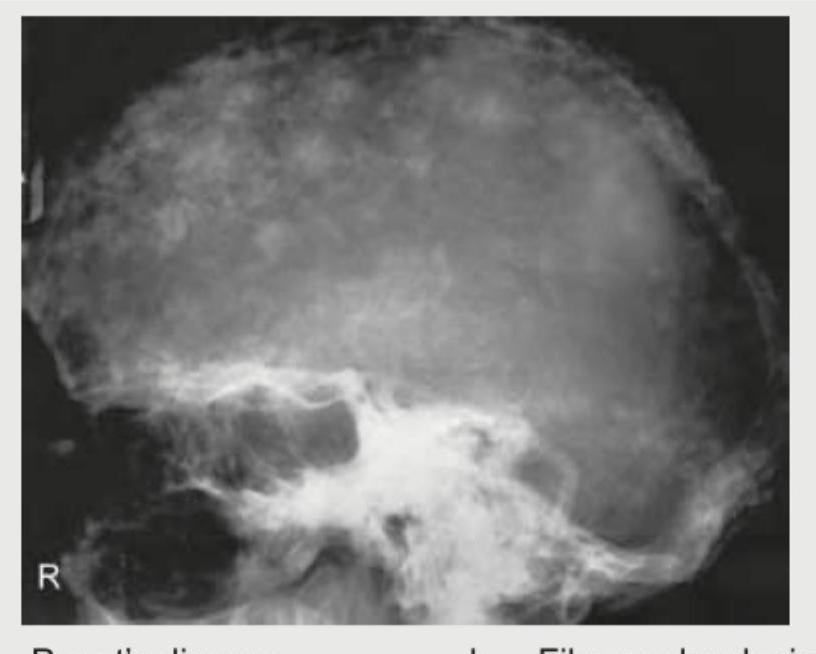
A 65-year-old man presents with bone pains. X-ray Skull shows? (Recent NEET Pattem 2018-19)
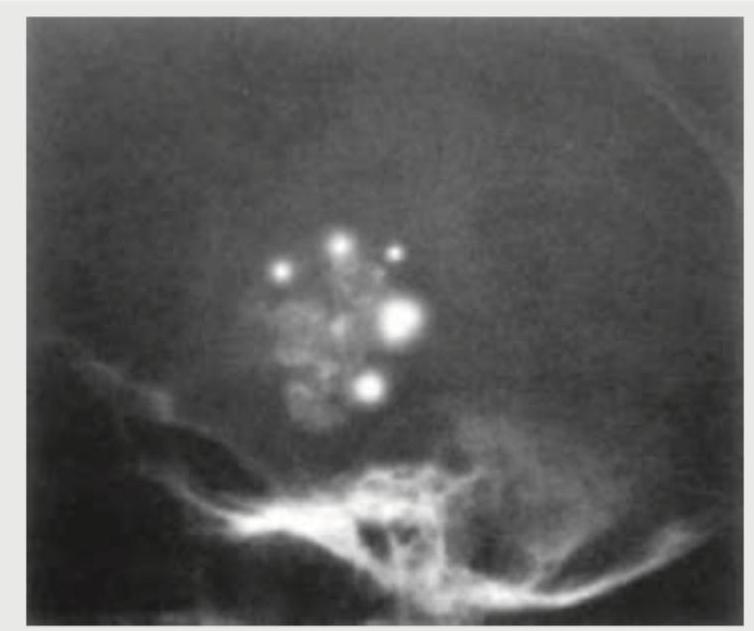
Q15
A 9-year-old female child presents with history of headache and visual disturbances. X-Ray skull is shown below. What is the possible diagnosis? (Recent NEET Pattern 2018-19)
Q16
Identify the structure shown in CT abdomen section. (Recent NEET Pattern 2018-19)
Q17
A 32-year-old lady presents with history of first trimester miscarriage and underwent HSG. The diagnosis is: (Recent NEET Pattern 2018-19)

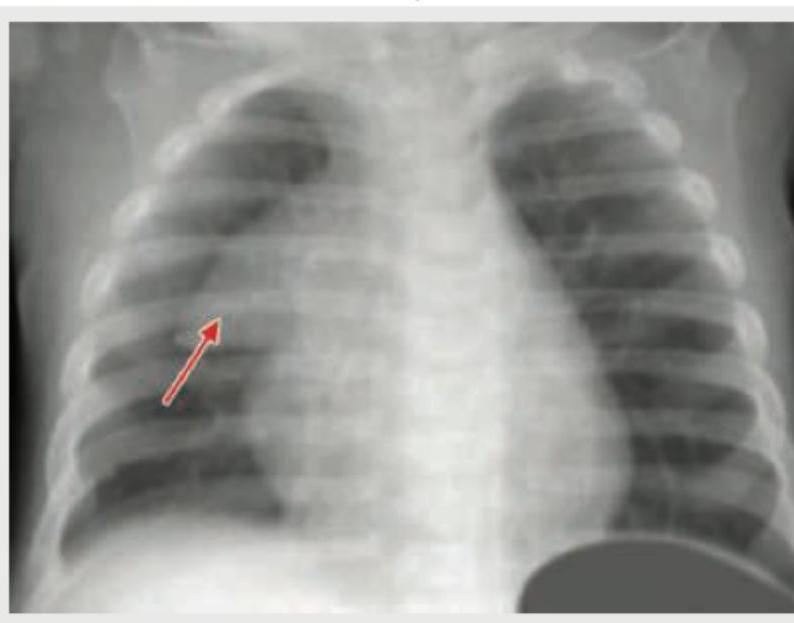
Q18
Comment on the arrow marked structure in CXR of an infant: (Recent NEET Pattern 2018-19)
Q19
The following Skull X-ray is seen in:
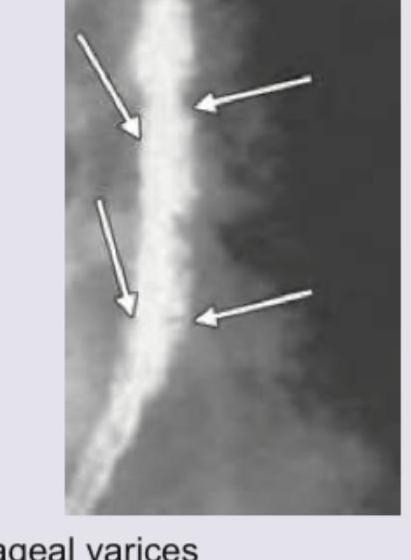
Q20
The following barium swallow study shows which of the following?