NEET-PG 2018 — Radiology
30 Previous Year Questions with Answers & Explanations
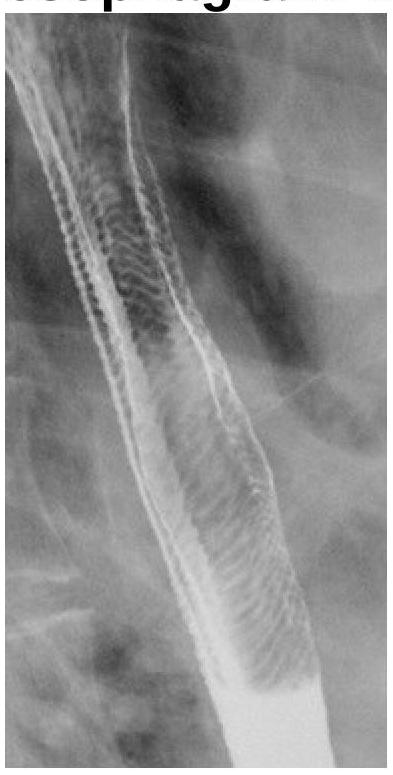
What does the following radiograph from a double contrast esophagram represent?
Water’s view is used to obtain diagnostic information of:
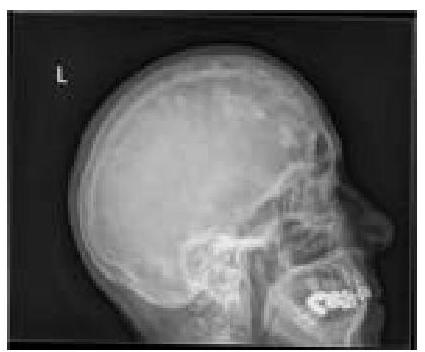
What type of lesions in the skull bones can be identified on this X-ray?

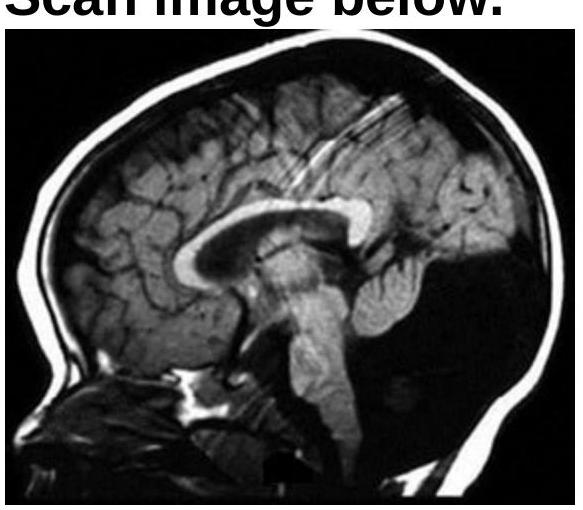
Which of the following abnormalities is most commonly detected as a vascular malformation on skull MRI?
What is the structure seen in the X-ray?

Identify the condition shown in the CT scan image.
What does the fallen fragment sign indicate in radiology?

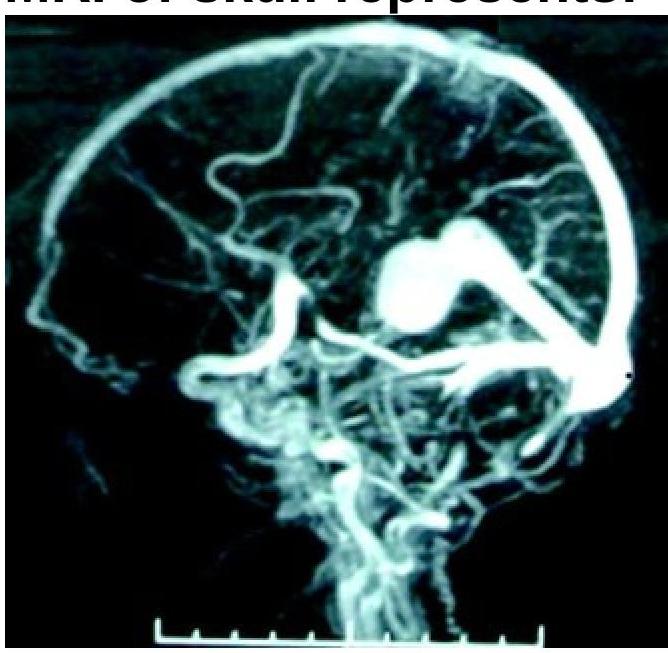
What condition is shown in the MR angiogram of the skull?
What type of lesions in the skull calvarium can be identified on this X-ray?
What is the diagnosis based on the following X-ray?

NEET-PG 2018 - Radiology NEET-PG Practice Questions and MCQs
Question 1: What does the following radiograph from a double contrast esophagram represent?
- A. Esophageal atresia
- B. Esophageal stenosis
- C. Feline esophagus (Correct Answer)
- D. Tracheoesophageal fistula
Explanation: **Feline esophagus (Correct)** - The image displays a characteristic transverse striation pattern along the esophageal mucosa, resembling the rings seen in the esophagus of a cat (hence "feline esophagus") - This finding is often associated with gastroesophageal reflux disease (GERD) or eosinophilic esophagitis, representing mucosal edema and inflammation - Also known as "ringed esophagus" or "corrugated esophagus" *Esophageal atresia (Incorrect)* - This is a congenital condition where the esophagus ends in a blind pouch, making it impossible for food to reach the stomach - The radiograph clearly shows a patent esophagus with contrast flowing through it, which rules out atresia *Esophageal stenosis (Incorrect)* - Esophageal stenosis refers to a narrowing of the esophagus, which would appear as a constricted segment on a barium swallow - While there is some irregularity, the primary pattern seen is transverse rings, not a focal, sustained narrowing typical of stenosis *Tracheoesophageal fistula (Incorrect)* - A tracheoesophageal fistula is an abnormal connection between the esophagus and the trachea - This would typically present with aspiration of contrast into the trachea or lungs, which is not evident in the provided image
Question 2: Water’s view is used to obtain diagnostic information of:
- A. Maxillary sinus (Correct Answer)
- B. Ethmoidal sinuses
- C. Frontal sinus
- D. Sphenoid sinus
Explanation: ***Maxillary sinus*** - **Water's view** (occipitomental projection) is specifically designed to visualize the **maxillary sinuses** and highlight any **fluid levels** or **mucosal thickening** within them. - In this view, the **petrous ridges are projected below the floors of the maxillary sinuses**, allowing for clear assessment and optimal visualization. *Ethmoidal sinuses* - While partially visible on Water's view, the **ethmoidal sinuses** are best visualized with a **Caldwell view** (occipitofrontal projection) or a **CT scan**. - The complex bony structures surrounding them make detailed assessment difficult with Water's view alone. *Frontal sinus* - The **frontal sinuses** are best evaluated with a **Caldwell view** (occipitofrontal projection), which projects the petrous ridges at the lower third of the orbits. - Water's view offers a suboptimal projection for comprehensive assessment of the frontal sinuses. *Sphenoid sinus* - The **sphenoid sinus** is centrally located and often obscured by other structures on plain radiographs like Water's view. - It is best visualized with a **lateral skull view** or, more comprehensively, with a **CT scan**.
Question 3: What type of lesions in the skull bones can be identified on this X-ray?
- A. Paget's disease (Correct Answer)
- B. Multiple myeloma
- C. Osteosarcoma
- D. Osteomyelitis
Explanation: ***Paget's disease*** - An X-ray of the skull in Paget's disease typically shows **thickening of the skull vault** and areas of both **osteolysis** and **osteosclerosis**, leading to a characteristic "cotton wool" appearance. - The disease involves abnormal bone remodeling, leading to enlarged and weakened bones susceptible to deformity and fracture. *Multiple myeloma* - On a skull X-ray, multiple myeloma usually presents as multiple, sharply-defined, **"punched-out" lytic lesions** without a sclerotic border. - These lesions reflect areas where malignant plasma cells have destroyed bone, which is distinct from the mixed lytic and sclerotic changes of Paget's disease. *Osteosarcoma* - Osteosarcoma is a **primary bone malignancy** that typically presents as a solitary lesion with a mixture of lytic and sclerotic areas, often with a **sunburst or Codman's triangle** periosteal reaction. - It most commonly affects long bones in younger individuals and is a much less common presentation in the skull compared to other bone conditions. *Osteomyelitis* - Osteomyelitis is an **infection of the bone** that would appear on an X-ray as areas of bone destruction (lysis) and new bone formation (sclerosis), often with **sequestrum** (dead bone) and **involucrum** (new bone formation around the infection). - While it can affect the skull, its imaging features would typically be localized signs of infection rather than the widespread, generalized changes seen in Paget's disease.
Question 4: Which of the following abnormalities is most commonly detected as a vascular malformation on skull MRI?
- A. Vein of Galen abnormalities (Correct Answer)
- B. Dandy Walker malformation
- C. Pneumocephalus presence
- D. Crouzon syndrome features
Explanation: ***Vein of Galen abnormalities*** - **Vein of Galen malformations (VOGM)** are the **most common symptomatic cerebral vascular malformations in neonates and infants**, accounting for approximately **30% of pediatric cerebral vascular malformations**. - They often present with **high-output cardiac failure**, hydrocephalus, or seizures in early life. - On **MRI**, they appear as a large, abnormal midline venous pouch in the quadrigeminal cistern with characteristic **flow voids** on T2-weighted images. - VOGM represents an **arteriovenous shunt** to a persistent embryonic vein (median prosencephalic vein of Markowski). *Dandy Walker malformation* - This is a **congenital brain malformation** involving the cerebellum and fourth ventricle, characterized by hypoplasia of the cerebellar vermis, cystic dilatation of the fourth ventricle, and an enlarged posterior fossa. - While readily seen on MRI, it is a **structural developmental anomaly**, not a vascular malformation. *Pneumocephalus presence* - **Pneumocephalus** refers to the presence of **air within the intracranial cavity**, usually resulting from trauma, neurosurgery, or skull base fractures. - It is an **acquired condition**, not a congenital vascular malformation, and appears as dark signal (air) on all MRI sequences. *Crouzon syndrome features* - **Crouzon syndrome** is a genetic disorder (FGFR2 mutation) characterized by **craniosynostosis** with premature fusion of coronal and sagittal sutures, leading to brachycephaly and midface hypoplasia. - It is a **craniofacial skeletal disorder**, not a vascular malformation.
Question 5: What is the structure seen in the X-ray?
- A. Stent (Correct Answer)
- B. Surgical clips
- C. Foley catheter
- D. Intravesical wire
Explanation: ***Stent*** - The image clearly shows **bilateral coiled structures** (pigtails) at the proximal and distal ends within the renal pelvis and bladder, which are characteristic features of **double J stents (ureteral stents)**. - These devices are used to maintain patency in the **ureters**, often to bypass obstructions or facilitate urine drainage. *Surgical clips* - **Surgical clips** are typically small, dense, metallic objects used to ligate vessels or tissue, appearing as tiny, bright specks on X-rays. - The structures seen in the image are long, tubular, and coiled, which is inconsistent with the appearance of surgical clips. *Foley catheter* - A **Foley catheter** is a flexible tube inserted into the bladder to drain urine, sometimes with a balloon tip. - It would typically be seen entirely within the **bladder**, and its path would not extend bilaterally into the renal pelvis as shown. *Intravesical wire* - An **intravesical wire** (a wire entirely within the bladder) would appear as a coiled or linear structure confined to the bladder itself. - The structures in the image extend from the renal region down into the bladder, traversing the **ureters**, which is not typical for an intravesical wire.
Question 6: Identify the condition shown in the CT scan image.
- A. None of the options
- B. Dandy-Walker malformation (Correct Answer)
- C. Cerebellar vermis hypoplasia
- D. Mega cisterna magna
Explanation: ***Dandy-Walker malformation*** - The image shows an enlarged posterior fossa with **cystic dilation of the fourth ventricle** and **absence/hypoplasia of the cerebellar vermis**, which are classic features of Dandy-Walker malformation. - The elevated tentorium and upward displacement of the transverse sinuses are also characteristic, contributing to the distinct appearance. *Cerebellar vermis hypoplasia* - While cerebellar vermis hypoplasia is a component of Dandy-Walker malformation, it is not the sole, defining feature. - Dandy-Walker also includes cystic dilation of the fourth ventricle and an enlarged posterior fossa, which are evident in the image and go beyond isolated vermis hypoplasia. *Mega cisterna magna* - A **mega cisterna magna** is a benign enlargement of the cisterna magna, which is the space between the cerebellum and the medulla oblongata. - Unlike in Dandy-Walker malformation, a mega cisterna magna usually does not involve displacement of the tentorium or hypoplasia of the cerebellar vermis, and the fourth ventricle is typically normal in shape and size. *None of the options* - The image clearly displays the diagnostic hallmarks of Dandy-Walker malformation, making this option incorrect.
Question 7: What does the fallen fragment sign indicate in radiology?
- A. Indicates a simple bone cyst (Correct Answer)
- B. Indicates osteosarcoma
- C. Indicates an aneurysmal bone cyst
- D. Indicates adamantinoma
Explanation: ***Indicates a simple bone cyst*** - The **fallen fragment sign** is a classic radiographic finding seen in **simple bone cysts** (unicameral bone cysts), particularly after a pathological fracture. - It occurs when a **fractured piece of bone** falls through the fluid-filled cyst cavity due to gravity, creating a characteristic appearance that indicates a benign, fluid-filled lesion. - This sign is considered **pathognomonic** for simple bone cysts. *Indicates osteosarcoma* - Osteosarcoma is a **malignant bone tumor** characterized by aggressive bone destruction and **osteoid formation**. - It typically does not demonstrate a fallen fragment sign; instead, it often shows a **Codman triangle** or **sunburst periosteal reaction**. - The aggressive nature and solid tumor composition make this sign incompatible with osteosarcoma. *Indicates an aneurysmal bone cyst* - An aneurysmal bone cyst (ABC) is a **benign, vascular bone lesion** that is usually multiloculated and blood-filled. - While it can cause bone expansion and pathological fractures, the fallen fragment sign is **not characteristic** of ABCs, which are typically hemorrhagic and contain blood-filled septa rather than clear fluid. - ABCs show a characteristic **fluid-fluid level** on imaging, not a fallen fragment. *Indicates adamantinoma* - Adamantinoma is a **rare, low-grade malignant bone tumor** most commonly found in the tibia. - This tumor does not exhibit a fallen fragment sign; its radiographic features often include **lobulated osteolytic lesions** with a sclerotic rim. - It is a solid tumor without the fluid-filled cavity necessary for this sign.
Question 8: What condition is shown in the MR angiogram of the skull?
- A. Vein of Galen malformation (Correct Answer)
- B. Dandy-Walker malformation
- C. Pneumocephalus
- D. Crouzon syndrome
Explanation: ***Vein of Galen malformation*** - The image provided is an **MR angiogram (MRA)**, which clearly shows a **large, dilated vein of Galen**. This is the characteristic appearance of a Vein of Galen malformation. - This congenital vascular malformation involves a direct artery-to-vein shunt, leading to the characteristic aneurysmal dilatation of the vein. *Dandy-Walker malformation* - This is a congenital brain malformation characterized by **agenesis or hypoplasia of the cerebellar vermis** and cystic dilation of the fourth ventricle. - While it affects brain structures, it does not involve the type of vascular abnormality seen in the image. *Pneumocephalus* - **Pneumocephalus** refers to the presence of **air within the intracranial cavity**, often due to trauma or surgery. - It would appear as dark areas on imaging, representing air, not the bright, dilated vascular structures seen here. *Crouzon syndrome* - **Crouzon syndrome** is a genetic disorder characterized by **craniosynostosis**, which is the premature fusion of skull sutures. - This condition primarily affects bone growth and skull shape, with no direct involvement of the cerebral vasculature as depicted in the MRA.
Question 9: What type of lesions in the skull calvarium can be identified on this X-ray?
- A. Brain metastases (Correct Answer)
- B. Multiple myeloma
- C. Osteosarcoma
- D. Osteomyelitis
Explanation: ***Brain metastases (Skull metastases)*** - The image shows multiple **lytic lesions** in the skull calvarium, which are characteristic of metastatic disease that has spread to bone - Metastases from primary cancers (lung, breast, kidney, thyroid, prostate) commonly involve the skull and appear as **punched-out or moth-eaten lytic lesions** - While plain X-rays cannot visualize brain parenchyma, they can detect **bony destruction** caused by metastatic deposits in the skull - These appear as well-defined osteolytic lesions without sclerotic margins *Multiple myeloma* - Multiple myeloma typically presents with **multiple punched-out lytic lesions** in the skull that can appear very similar to metastases - However, multiple myeloma is a **primary bone marrow malignancy** rather than metastatic disease - Key differentiator: myeloma lesions are usually more uniform in size and distribution - Clinical context (monoclonal protein, anemia, renal dysfunction) helps distinguish from metastases *Osteosarcoma* - Osteosarcoma is a **primary bone tumor** that usually causes a mixture of lytic and blastic (bone-forming) lesions - Typically presents with **sunburst or spiculated periosteal reaction** and soft tissue mass - Usually occurs as a **solitary aggressive lesion** in younger patients, not multiple scattered lesions - Rarely occurs in the skull compared to long bones *Osteomyelitis* - Osteomyelitis is an **infection of the bone** that causes bone destruction and reactive new bone formation - Shows features of **bone destruction, periosteal reaction**, and possibly sequestra (dead bone fragments) - Typically presents as a **focal process** with surrounding inflammatory changes - Does not produce the multiple discrete lytic lesions pattern seen in metastatic disease
Question 10: What is the diagnosis based on the following X-ray?
- A. Bladder Stone
- B. Renal Tuberculosis (Correct Answer)
- C. Uterine Fibroid
- D. Bladder Carcinoma
Explanation: ***Renal Tuberculosis*** - Characterized by **calcifications** in the renal parenchyma and collecting system visible on X-ray, often appearing as **moth-eaten** or **amputated calyces** - Associated with **sterile pyuria**, **acidic urine**, and **caseous necrosis** leading to characteristic radiographic findings of calcified granulomas *Uterine Fibroid* - Appears as a **well-defined soft tissue mass** arising from the pelvis, often with **popcorn calcifications** if degenerating - Located in the **uterine region** rather than the renal area, and typically presents with menstrual abnormalities and pelvic pressure *Bladder Carcinoma* - Presents as an **irregular filling defect** or **mass** within the bladder on contrast studies, rarely with calcifications - Associated with **hematuria** and typically shows **soft tissue density** rather than the dense calcifications seen in renal TB *Bladder Stone* - Appears as a **rounded, smooth radiopaque density** in the pelvis corresponding to the bladder location - Usually has a **homogeneous density** with well-defined borders, unlike the irregular calcifications of renal tuberculosis