NEET-PG 2018 — Physiology
13 Previous Year Questions with Answers & Explanations
In hypovolemic shock there is -
What happens to gas exchange when the Va/Q ratio approaches infinity?
What is the physiological response of the kidney during shock?
Nude mice are not resistant to xenografts due to absence of
Insulin-like growth factor is secreted by:
Which of the following is endogenous pyrogen?
Glucose is absorbed in the intestine by?
In a child with suspected tetany, the following test is performed. Identify the sign?
Which ion plays a role in the process shown below? (Recent NEET Pattern 2018)
Which of the following is not a component of the process shown in the image?
NEET-PG 2018 - Physiology NEET-PG Practice Questions and MCQs
Question 1: In hypovolemic shock there is -
- A. Efferent arteriolar constriction
- B. Increased blood flow to kidney
- C. Decreased cardiac output (Correct Answer)
- D. Afferent arteriolar constriction
Explanation: ***Decreased cardiac output*** - **Hypovolemic shock** is fundamentally defined by **decreased circulating blood volume**, which leads to **decreased venous return** to the heart. - According to the **Frank-Starling mechanism**, decreased venous return leads to **decreased preload**, which results in **decreased stroke volume** and consequently **decreased cardiac output**. - This is the **primary hemodynamic characteristic** of hypovolemic shock and is present in ALL cases. - Decreased cardiac output triggers all the compensatory mechanisms seen in hypovolemic shock, including sympathetic activation and RAAS activation. *Afferent arteriolar constriction* - While afferent arteriolar constriction does occur in hypovolemic shock due to **sympathetic activation**, it is a **compensatory response** rather than the primary feature. - The predominant effect at the kidney level is actually a combination of both afferent and efferent arteriolar changes. - This occurs secondary to the decreased cardiac output. *Efferent arteriolar constriction* - **Efferent arteriolar constriction** is mediated primarily by **angiotensin II** and is actually MORE prominent than afferent constriction. - This helps **maintain glomerular filtration rate (GFR)** despite reduced renal blood flow by increasing glomerular hydrostatic pressure. - However, this is also a compensatory response, not the primary feature of hypovolemic shock. *Increased blood flow to kidney* - This is incorrect as hypovolemic shock causes **decreased renal blood flow**. - Blood is redistributed away from the kidneys to vital organs like the heart and brain through compensatory vasoconstriction.
Question 2: What happens to gas exchange when the Va/Q ratio approaches infinity?
- A. Partial pressure of O2 becomes negligible.
- B. No exchange of O2 and CO2 occurs. (Correct Answer)
- C. Partial pressure of CO2 becomes negligible.
- D. Partial pressures of both CO2 and O2 remain normal.
Explanation: ***No exchange of O2 and CO2 occurs.*** - When the **Va/Q ratio approaches infinity**, it signifies a scenario of **ventilation without perfusion** (Q approaches zero). - This represents **alveolar dead space** - despite adequate ventilation, there is **no blood flow** to participate in gas exchange. - Therefore, **no O2 enters the blood** and **no CO2 leaves the blood**, making this the most accurate description of what happens to gas exchange. *Partial pressure of O2 becomes negligible.* - This statement is incorrect because with **no blood flow** (Q = 0), the alveolar air retains high O2 partial pressure. - O2 is being delivered via ventilation but not removed by blood, so **alveolar PO2** would approach that of **inspired air (~150 mmHg)**, not become negligible. *Partial pressure of CO2 becomes negligible.* - While this statement is technically true (alveolar PCO2 would approach zero/inspired air levels), it doesn't directly answer what happens to **gas exchange**. - With no blood flowing through the alveolus, no **CO2 from venous blood** can reach the alveolus to be excreted. - However, the question asks about **gas exchange** itself, not just partial pressures, making the first option more comprehensive. *Partial pressures of both CO2 and O2 remain normal.* - This statement is incorrect as the **Va/Q mismatch** significantly alters the partial pressures of both gases. - In infinite Va/Q scenario (dead space ventilation), **alveolar PO2 would be high** (approaching inspired air ~150 mmHg) and **alveolar PCO2 would be low** (approaching zero).
Question 3: What is the physiological response of the kidney during shock?
- A. GFR decreases
- B. Perfusion of kidney decreases
- C. Afferent arteriole resistance increases
- D. Renal blood flow decreases (Correct Answer)
Explanation: ***Renal blood flow decreases*** - During shock, the **primary and most fundamental** physiological change affecting the kidney is a marked **reduction in renal blood flow (RBF)**. - Shock triggers intense **sympathetic activation** and **renin-angiotensin system (RAS) activation**, causing preferential **vasoconstriction** of renal vessels to redirect blood to vital organs (brain, heart). - RBF can drop to as low as **20-30% of normal** in severe shock, making this the hallmark renal response. - This reduction in RBF is the **upstream event** that triggers all other renal changes during shock. *Perfusion of kidney decreases* - While technically correct, "decreased perfusion" is **essentially synonymous** with decreased blood flow in this context. - The term "renal blood flow" is the **standard physiological terminology** used in medical literature to describe this phenomenon, making it the more precise answer. *Afferent arteriole resistance increases* - This is a **mechanism** by which RBF decreases, not the overall response itself. - Increased afferent arteriolar resistance is **secondary** to sympathetic activation and angiotensin II effects during shock. - It describes the "how" rather than the "what" of the kidney's response. *GFR decreases* - GFR reduction is a **consequence** of decreased RBF and increased afferent arteriolar resistance. - While clinically important (oliguria/acute kidney injury), it's a **downstream effect** rather than the primary physiological response. - The relationship: ↓RBF → ↓Glomerular hydrostatic pressure → ↓GFR
Question 4: Nude mice are not resistant to xenografts due to absence of
- A. B cell
- B. T cell (Correct Answer)
- C. Absence of both B and T cells
- D. Presence of both B and T cells
Explanation: ***T cell*** - Nude mice have a **congenital athymia**, meaning they lack a functional **thymus**. - The thymus is essential for the maturation and development of **T lymphocytes**, making these mice severely **T-cell deficient**. - Without functional T cells, nude mice cannot reject **xenografts** (tissue transplanted from a different species). *B cell* - While nude mice have impaired T-cell function, their **B-cell development and function remain largely intact**. - B cells develop in the **bone marrow** and do not require the thymus for maturation. - B cells alone are insufficient to reject xenografts, as this requires cell-mediated immunity. *Absence of both B and T cells* - This statement is incorrect because nude mice **do possess B cells**, even if their T-cell immunity is severely compromised. - The primary defect is in the **thymus**, affecting T-cell maturation, not B cells. - Complete absence of both would describe **SCID mice**, not nude mice. *Presence of both B and T cells* - This is incorrect as nude mice clearly have a **severe deficiency in T cells** due to athymia. - Their inability to reject xenografts is directly linked to this lack of functional T-cell immunity. - If both were present and functional, the mice would reject xenografts normally.
Question 5: Insulin-like growth factor is secreted by:
- A. Liver (Correct Answer)
- B. Pituitary gland
- C. Pancreas
- D. Adrenal glands
Explanation: ***Liver*** - The **liver** is the primary site of **insulin-like growth factor 1 (IGF-1)** production in response to **growth hormone (GH)** stimulation. - IGF-1 mediates many of the growth-promoting effects of GH, affecting various tissues throughout the body. *Pituitary gland* - The **pituitary gland** secretes **growth hormone (GH)**, which then stimulates the liver to produce IGF-1, but it does not directly secrete IGF-1. - Its role is upstream in the GH-IGF-1 axis, initiating the signaling cascade. *Pancreas* - The **pancreas** is primarily known for secreting **insulin** and **glucagon**, which regulate blood glucose levels. - It does not produce significant amounts of IGF-1. *Adrenal glands* - The **adrenal glands** produce hormones like **cortisol**, **aldosterone**, and **androgens**. - They are not involved in the direct secretion of IGF-1.
Question 6: Which of the following is endogenous pyrogen?
- A. PG E2 (Correct Answer)
- B. PG D2
- C. PGF2 alpha
- D. PG I2
Explanation: ***PG E2*** - **Prostaglandin E2 (PGE2)** is considered the **endogenous mediator of fever** in the context of this question (NEET-PG 2018). - **Mechanism:** PGE2 acts on the **preoptic area of the hypothalamus** to raise the body's temperature set point, leading to fever. - **Production pathway:** Endogenous pyrogens like **IL-1, IL-6, and TNF-α** stimulate **cyclooxygenase-2 (COX-2)** in hypothalamic endothelial cells → **PGE2 synthesis** → binds to EP3 receptors → raises set point. - **Clinical relevance:** This is why **antipyretics** (aspirin, paracetamol, NSAIDs) work by inhibiting COX enzymes, thereby reducing PGE2 production. - **Terminology note:** Strictly speaking, cytokines (IL-1, IL-6, TNF-α) are the true "endogenous pyrogens," while PGE2 is the "final common mediator" - but for exam purposes, PGE2 is accepted as the endogenous pyrogenic mediator. *PG D2* - **Prostaglandin D2 (PGD2)** is primarily involved in **allergic reactions**, **sleep regulation**, and modulating immune responses. - Main roles include **bronchoconstriction** in asthma, **vasodilation**, and mast cell activation. - It does **not** act as a fever mediator in the hypothalamus. *PGF2 alpha* - **Prostaglandin F2 alpha (PGF2α)** functions primarily in **reproductive physiology**. - Causes **uterine contractions** (labor induction), **luteolysis** (corpus luteum regression), and **bronchoconstriction**. - It has **no direct role** in fever generation or thermoregulation. *PG I2* - **Prostacyclin (PGI2)** is a potent **vasodilator** and **inhibitor of platelet aggregation**. - Produced by vascular endothelium, it has **anti-thrombotic** and **anti-inflammatory** properties. - It does **not** function as a pyrogenic mediator and may actually have **antipyretic effects** in some contexts.
Question 7: Glucose is absorbed in the intestine by?
- A. Facilitated diffusion
- B. Simple diffusion
- C. Secondary active transport (Correct Answer)
- D. Primary active transport
Explanation: ***Secondary active transport*** - Glucose absorption in the intestine primarily occurs via the **SGLT1 (sodium-glucose cotransporter 1)** protein. - SGLT1 uses the **electrochemical gradient of sodium** (established by Na+/K+-ATPase) to co-transport glucose against its concentration gradient, classifying it as secondary active transport. *Facilitated diffusion* - While **facilitated diffusion** by GLUT2 transporters is involved in glucose exit from the intestinal cells into the bloodstream, it's not the primary mechanism for uptake from the lumen. - This process does not require direct energy expenditure, but relies on a **concentration gradient**. *Simple diffusion* - **Simple diffusion** involves the movement of substances directly across the membrane, down their concentration gradient, without the help of transport proteins. - Glucose is a **hydrophilic molecule** and too large to pass through the lipid bilayer by simple diffusion. *Primary active transport* - **Primary active transport** directly uses ATP hydrolysis to move substances against their concentration gradient (e.g., Na+/K+-ATPase). - While essential for maintaining the sodium gradient, it is not the direct mechanism for glucose uptake from the intestinal lumen.
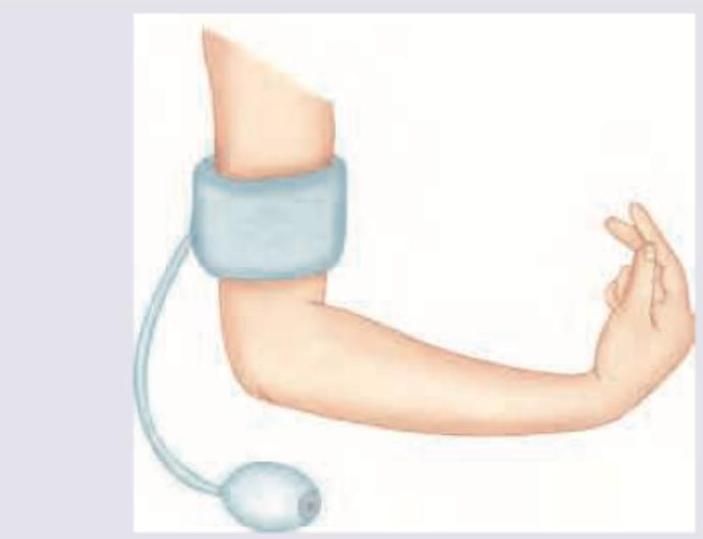
Question 8: In a child with suspected tetany, the following test is performed. Identify the sign?
- A. Chvostek sign
- B. Allen sign
- C. Trousseau sign (Correct Answer)
- D. Turner sign
Explanation: ***Trousseau sign*** - The image depicts a blood pressure cuff inflated on the arm, leading to **carpopedal spasm** in the hand, which is characteristic of the **Trousseau sign**. - This sign is indicative of **latent tetany** and is often seen in conditions causing **hypocalcemia**. *Chvostek sign* - The Chvostek sign involves a **facial muscle twitch** elicited by tapping the facial nerve anterior to the ear. - This sign is also associated with hypocalcemia but differs clinically from the presentation in the image. *Allen sign* - The Allen test (not "sign") is performed to assess the **patency of the ulnar and radial arteries** before arterial puncture or cannulation. - It involves digitally compressing both arteries and observing the return of color to the hand after releasing one artery, which is unrelated to the image. *Turner sign* - The Turner sign refers to **flank ecchymosis** (bruising) and is a physical finding associated with **hemorrhagic pancreatitis**. - This sign indicates retroperitoneal bleeding, which is not represented by the image or related to tetany.
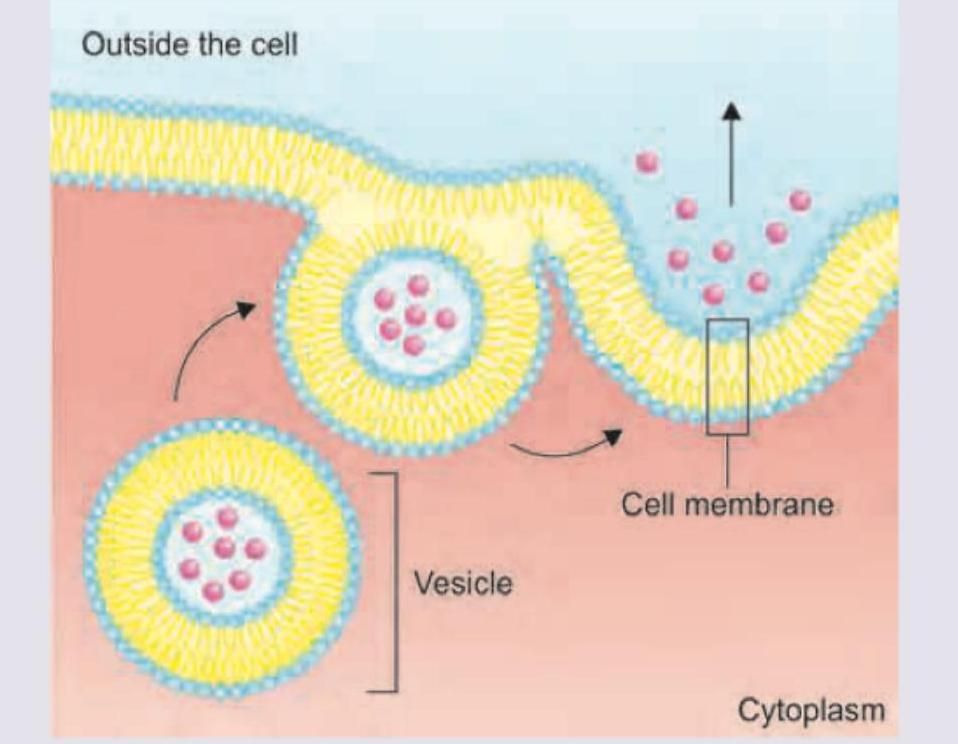
Question 9: Which ion plays a role in the process shown below? (Recent NEET Pattern 2018)
- A. Potassium
- B. Sodium
- C. Magnesium
- D. Calcium (Correct Answer)
Explanation: ***Calcium*** - **Calcium ions (Ca2+)** are the primary trigger for **exocytosis**, binding to **synaptotagmin** proteins on synaptic vesicles to initiate membrane fusion. - Ca2+ influx activates the **SNARE complex** formation, allowing vesicles to fuse with the plasma membrane and release neurotransmitters or other cellular contents. *Potassium* - **Potassium ions (K+)** are primarily responsible for maintaining the **resting membrane potential** and **repolarization** during action potentials. - While essential for neuronal function, K+ does not directly trigger **vesicle fusion** or exocytosis processes. *Sodium* - **Sodium ions (Na+)** are crucial for **action potential depolarization** and maintaining **electrochemical gradients** across cell membranes. - Na+ influx initiates nerve impulses but does not serve as the direct trigger for **vesicle release** during exocytosis. *Magnesium* - **Magnesium ions (Mg2+)** function as essential **cofactors** for numerous enzymes and play roles in **ATP metabolism** and **protein synthesis**. - Although Mg2+ can modulate some cellular processes, it is not the primary ion responsible for triggering **exocytotic release**.
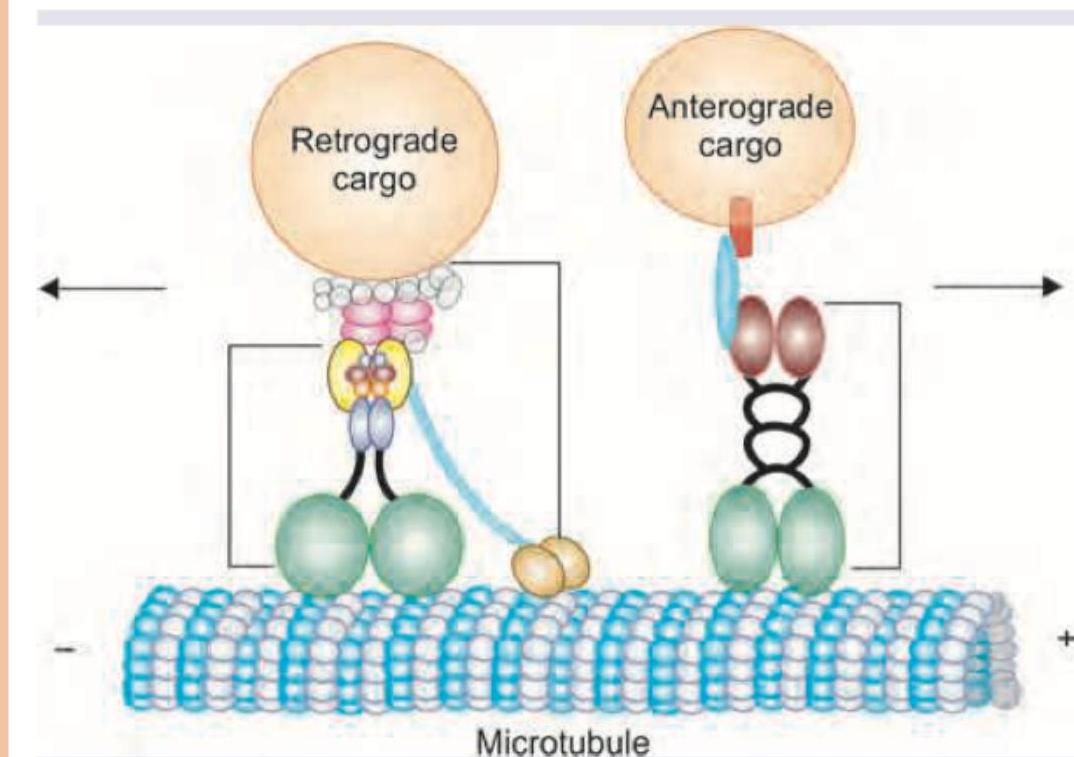
Question 10: Which of the following is not a component of the process shown in the image?
- A. Dynein
- B. Kinesin
- C. Myosin
- D. Actin (Correct Answer)
Explanation: ***Actin*** - The image depicts **microtubule-based transport** involving motor proteins (dynein and kinesin) moving cargo along microtubules. - **Actin filaments** are a completely separate cytoskeletal system and are NOT components of the microtubule-based process shown. - This is the most fundamental distinction - actin vs. microtubule cytoskeletal systems. *Dynein* - **Dynein** is clearly shown in the image, transporting **retrograde cargo** toward the minus end of the microtubule. - It is a key motor protein for minus-end directed movement along microtubules. *Kinesin* - **Kinesin** is depicted in the image, transporting **anterograde cargo** toward the plus end of the microtubule. - It is the primary motor protein for plus-end directed movement along microtubules. *Myosin* - While **myosin** typically works with actin filaments rather than microtubules, it belongs to the same functional category as dynein and kinesin (motor proteins). - Some myosin isoforms can even associate with microtubule-based processes in specific contexts. - **Actin** is the better answer as it represents a completely different cytoskeletal system, whereas myosin is still a motor protein like the others listed.