NEET-PG 2018 — Pediatrics
24 Previous Year Questions with Answers & Explanations
What is a key diagnostic criterion for acute respiratory distress syndrome (ARDS) in a child?
A child has a rash. His family history is positive for asthma. What could be the most probable diagnosis?

A 1-year-old child weighing 6 kg is suffering from acute gastroenteritis with signs of sunken eyes and skin pinch returning to normal very rapidly. What will be your management?
Which of the following is NOT included in the resuscitation of a neonate with HR < 60/min?
Which of the following diseases will lead to the following appearance?
Neonate is brought at 3 weeks of age, with projectile vomiting. USG was performed and is shown below. When can the abdominal mass in this condition be best palpated?
A 1-year-old child with severe acute malnutrition develops pneumonia which is not responding to treatment. Chest X-ray picture is given. What is the likely etiology?
A 12-month-old child who was previously well presented with low grade fever and respiratory distress and on examination there is bilateral wheeze. There is a history of URI in elder sibling. What is the diagnosis?
A child with history of diarrhea 1 week back presents with sudden onset pallor and oliguria. Peripheral smear findings are shown below. Which of the following is unlikely finding in this disorder?
A child during evaluation of recurrent hematuria has the following eye finding. He has sensorineural deafness and history of similar illness in family members. What is the diagnosis?
NEET-PG 2018 - Pediatrics NEET-PG Practice Questions and MCQs
Question 1: What is a key diagnostic criterion for acute respiratory distress syndrome (ARDS) in a child?
- A. Within 7 days of known clinical insult (Correct Answer)
- B. Respiratory failure not fully explained
- C. Left ventricular dysfunction
- D. All of the options
Explanation: ***Within 7 days of known clinical insult*** - A key diagnostic criterion for **Acute Respiratory Distress Syndrome (ARDS)** in children is the onset of respiratory symptoms within **7 days of a known clinical insult**. - This temporal relationship helps distinguish ARDS from other causes of respiratory failure that may have a more chronic or delayed onset. *Respiratory failure not fully explained* - **Respiratory failure not fully explained** by other conditions is a general characteristic but not a specific diagnostic criterion on its own. - ARDS requires the exclusion of cardiac failure as the primary cause of pulmonary edema, indicated by an absence of left atrial hypertension. *Left ventricular dysfunction* - **Left ventricular dysfunction** would suggest **cardiogenic pulmonary edema**, which needs to be excluded for a diagnosis of ARDS. - ARDS is characterized by **non-cardiogenic pulmonary edema**, meaning the fluid in the lungs is not due to heart failure. *All of the options* - This option is incorrect because **left ventricular dysfunction** is an *exclusion criterion* for ARDS, not a diagnostic criterion, as ARDS is defined by **non-cardiogenic pulmonary edema**. - While the other options relate to aspects of ARDS, only one is a key diagnostic criterion as formulated.
Question 2: A child has a rash. His family history is positive for asthma. What could be the most probable diagnosis?
- A. Seborrheic dermatitis
- B. Atopic dermatitis (Correct Answer)
- C. Allergic contact dermatitis
- D. Erysipelas
Explanation: ***Atopic dermatitis*** - The presence of a rash in a child with a family history of **asthma** strongly suggests atopic dermatitis, as it is part of the **atopic triad** (eczema, asthma, allergic rhinitis). - Atopic dermatitis often presents with **erythematous, pruritic patches** and plaques, commonly affecting flexural areas like the antecubital and popliteal fossae, as well as the face and neck in younger children. *Seborrheic dermatitis* - This condition typically presents with **greasy, yellowish scales** on an erythematous base, often affecting areas rich in sebaceous glands such as the scalp, face (nasolabial folds), and chest. - While it can occur in infants, it does not have the strong association with a family history of asthma seen in atopic dermatitis. *Allergic contact dermatitis* - This rash results from an **exposure to an allergen**, leading to a localized, erythematous, and pruritic eruption, often with vesicles or bullae, at the site of contact. - The history does not provide information about a specific allergen exposure, and while it could produce a similar-looking rash, the family history of asthma points more strongly to atopic diathesis. *Erysipelas* - Erysipelas is a superficial skin infection, usually caused by *Streptococcus pyogenes*, presenting as a **well-demarcated, intensely erythematous, warm, and painful rash** with a raised border. - This is an **acute bacterial infection** and would typically be accompanied by systemic symptoms like fever and chills, which are not mentioned in the child's presentation.
Question 3: A 1-year-old child weighing 6 kg is suffering from acute gastroenteritis with signs of sunken eyes and skin pinch returning to normal very rapidly. What will be your management?
- A. RL infusion 120 ml in the first hour followed by 360 ml in the next 5 hours
- B. RL infusion 180 ml in the first hour followed by 480 ml in the next 5 hours
- C. RL infusion 240 ml in the first hour followed by 360 ml in the next 5 hours
- D. RL infusion 180 ml in the first hour followed by 270 ml in the next 5 hours (Correct Answer)
Explanation: ***RL infusion 180 ml in the first hour followed by 270 ml in the next 5 hours*** - The child shows signs of **some dehydration** (sunken eyes, skin pinch returning very rapidly). According to **WHO Plan B**, some dehydration requires **75 ml/kg over 6 hours** for rehydration. - For a 6 kg child: **75 × 6 = 450 ml total** - **Distribution:** 30 ml/kg in first hour (180 ml) + 45 ml/kg over next 5 hours (270 ml) - This option provides exactly **450 ml (180 + 270)**, perfectly matching WHO guidelines for some dehydration *RL infusion 120 ml in the first hour followed by 360 ml in the next 5 hours* - First hour: 120 ml = only **20 ml/kg**, which is **below the recommended 30 ml/kg** initial bolus for some dehydration - Total volume: **480 ml** exceeds the required **450 ml** for a 6 kg child - Incorrect fluid distribution pattern for WHO Plan B *RL infusion 180 ml in the first hour followed by 480 ml in the next 5 hours* - First hour volume is correct at **30 ml/kg (180 ml)** - However, next 5 hours: **480 ml = 80 ml/kg**, far exceeding the recommended **45 ml/kg** - Total: **660 ml** significantly exceeds **450 ml**, risking **fluid overload** in a small child *RL infusion 240 ml in the first hour followed by 360 ml in the next 5 hours* - Initial rate: **240 ml = 40 ml/kg** is appropriate for **severe dehydration (WHO Plan C)**, not some dehydration - This child shows **some dehydration** signs, not severe (no lethargy, unconsciousness, or very slow skin pinch) - Total: **600 ml** exceeds the **450 ml** requirement, indicating overtreatment for this clinical scenario
Question 4: Which of the following is NOT included in the resuscitation of a neonate with HR < 60/min?
- A. Endotracheal tube intubation
- B. Chest compression
- C. Adrenaline
- D. None of the above (Correct Answer)
Explanation: ***None of the above*** - All listed interventions—**endotracheal tube intubation**, **chest compressions**, and **adrenaline administration**—are standard components of neonatal resuscitation when the heart rate remains below 60 beats/min despite initial steps. - This question asks which is *NOT* included, implying that all options are, in fact, appropriate interventions in this critical scenario. *Endotracheal tube intubation* - This is a critical step in **securing the airway** and ensuring effective positive pressure ventilation when other methods fail or prolonged mechanical ventilation is anticipated. - It's indicated if the heart rate remains below 60 bpm despite adequate bag-mask ventilation and chest compressions. *Chest compression* - **Chest compressions** are initiated when the heart rate is less than 60 bpm *after* 30 seconds of effective positive pressure ventilation. - They are used in conjunction with positive pressure ventilation to improve cardiac output and myocardial perfusion. *Adrenaline* - **Adrenaline** is administered if the heart rate remains below 60 bpm *despite* adequate ventilation and chest compressions. - It acts as a potent **vasopressor** and **cardiac stimulant**, increasing heart rate and contractility.
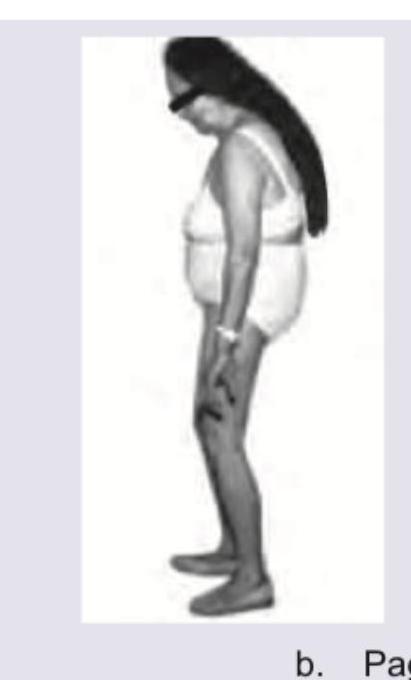
Question 5: Which of the following diseases will lead to the following appearance?
- A. Polio
- B. Paget's disease (Correct Answer)
- C. Cerebellar lesion
- D. Ankylosing Spondylitis
Explanation: ***Paget's disease*** - The image depicts a bowing of the legs and a generalized stooped posture, which are characteristic findings in advanced **Paget's disease of bone**. - **Paget's disease** is a chronic bone disorder characterized by abnormal bone remodeling, leading to enlarged and misshapen bones that can cause **kyphosis** and **bowed limbs**. *Polio* - **Polio** (poliomyelitis) primarily affects the nervous system, leading to **muscle weakness** and **paralysis**, which can result in limb deformities, but not typically the widespread bone enlargement and bowing seen here. - While polio can cause limb asymmetry and deformities due to muscle wasting, it does not involve the characteristic bone remodeling and generalized skeletal changes seen in the image. *Cerebellar lesion* - A **cerebellar lesion** primarily affects coordination, balance, and motor control, leading to ataxia, tremors, and gait disturbances. - It does not directly cause the skeletal deformities or bone bowing illustrated in the image. *Ankylosing Spondylitis* - **Ankylosing spondylitis** is a chronic inflammatory disease primarily affecting the axial skeleton, leading to progressive spinal stiffness and fusion (a "bamboo spine"). - While it can cause a significant **kyphosis** (forward curvature of the spine), it does not typically lead to the wide-set bowed legs or general bone enlargement often seen in Paget's disease.
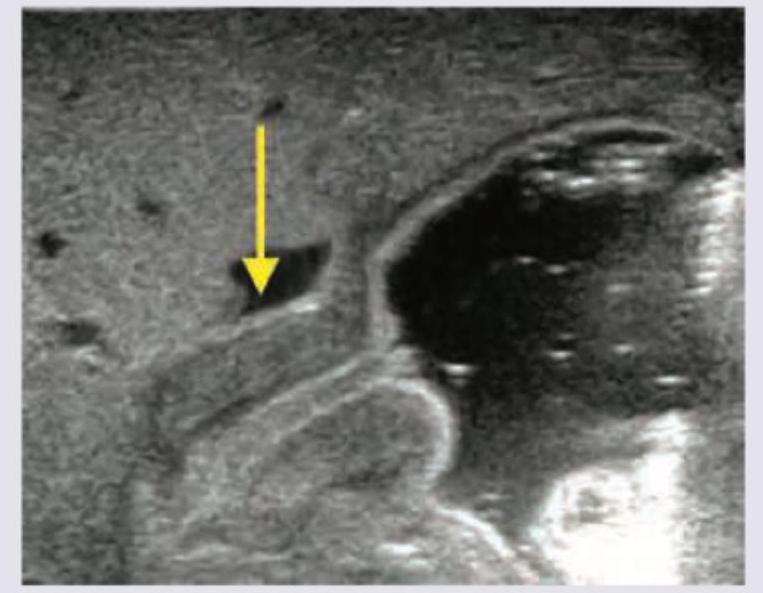
Question 6: Neonate is brought at 3 weeks of age, with projectile vomiting. USG was performed and is shown below. When can the abdominal mass in this condition be best palpated?
- A. During feeding (Correct Answer)
- B. In umbilical area
- C. In epigastric area
- D. In Right upper quadrant
Explanation: ***During feeding*** - In **hypertrophic pyloric stenosis**, the characteristic **"olive" mass** formed by the thickened pylorus is most easily palpable **during feeding or immediately after vomiting**. - During this time, the infant’s abdominal muscles are relaxed, making palpation of the mass in the **epigastrium (right upper quadrant)** more successful. *In umbilical area* - The umbilical area is typically where **omphaloceles** or **umbilical hernias** are found, not the pyloric mass. - The pylorus is located much higher in the epigastric region, to the right of the midline. *In epigastric area* - While the pyloric mass is located in the **epigastric area**, palpation is more difficult when the infant is crying or agitated. - The question asks when it can be *best* palpated, emphasizing the conditions under which it is most detectable. *In Right upper quadrant* - The pylorus is indeed located in the **right upper quadrant/epigastrium**. - However, the optimal timing for palpation is during feeding or after vomiting, as the infant's abdomen is relaxed at that point.
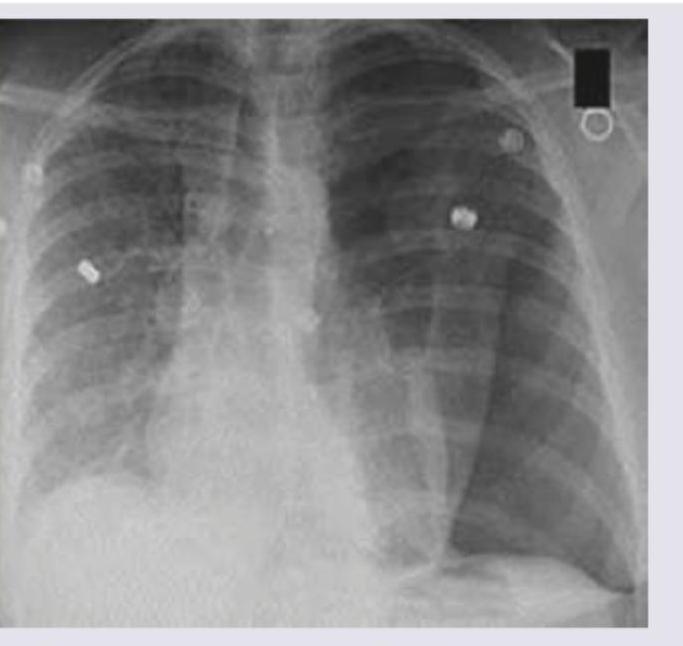
Question 7: A 1-year-old child with severe acute malnutrition develops pneumonia which is not responding to treatment. Chest X-ray picture is given. What is the likely etiology?
- A. Mycoplasma
- B. Pneumococcus
- C. Staphylococcus aureus (Correct Answer)
- D. Adenovirus
Explanation: ***Staphylococcus aureus*** - The chest X-ray shows extensive **bilateral infiltrates** with areas of potential **abscess formation** or **necrotizing pneumonia**, suggested by the poorly defined lucencies within consolidation, which are characteristic of Staphylococcal infection, especially in immunocompromised individuals like a malnourished child. - Staphylococcal pneumonia is often severe, can lead to **necrosis**, **cavitation**, and is known for its **resistance to common antibiotics**, explaining the poor response to initial treatment in a severely malnourished child. *Mycoplasma* - Mycoplasma pneumoniae typically causes **"walking pneumonia"** with milder symptoms and **diffuse interstitial infiltrates** visible on Chest X-ray, which are not as severe or focal as seen in the image. - It's less common to cause rapidly progressing, severe, and necrotizing pneumonia in this age group, even in malnourished children. *Pneumococcus* - **Streptococcus pneumoniae (Pneumococcus)** usually causes **lobar pneumonia** with dense, homogeneous consolidation in one lobe, often with a visible air bronchogram, rather than the more patchy, bilateral, and potentially necrotizing pattern seen here. - While it can be severe, especially in malnourished children, the radiographic pattern is less typical for pneumococcal infection. *Adenovirus* - Adenovirus can cause a range of respiratory infections, from common colds to severe pneumonia, especially in young children. However, the Chest X-ray findings typically include **perihilar infiltrates**, **bronchial wall thickening**, and hyperinflation, which do not fully match the extensive, severe, and potentially cavitating pattern observed. - While it can cause severe pneumonia, the given X-ray features, particularly the suggestion of necrosis, are less characteristic of adenoviral infection.
Question 8: A 12-month-old child who was previously well presented with low grade fever and respiratory distress and on examination there is bilateral wheeze. There is a history of URI in elder sibling. What is the diagnosis?
- A. Congestive cardiac failure
- B. Pneumonia
- C. Acute bronchiolitis (Correct Answer)
- D. Asthma exacerbation
Explanation: ***Acute bronchiolitis*** - The clinical presentation of a **12-month-old** with **low-grade fever**, **respiratory distress**, and **bilateral wheeze**, along with the history of a preceding **URI in an elder sibling**, is highly characteristic of acute bronchiolitis, commonly caused by **Respiratory Syncytial Virus (RSV)**. - Bronchiolitis primarily affects infants and toddlers, causing inflammation and obstruction of the small airways, leading to wheezing and increased work of breathing. - The **age (12 months)** and **contact history** are key diagnostic clues. *Congestive cardiac failure* - While congestive cardiac failure can cause respiratory distress, it typically presents with other signs like **tachycardia**, **hepatomegaly**, and potentially a cardiac murmur, which are not mentioned here. - Wheezing can occur in cardiac failure but is usually accompanied by **rales** and signs of fluid overload rather than prominent diffuse wheezing as the primary respiratory finding in an otherwise well child. *Pneumonia* - Pneumonia would more typically present with a **higher fever**, **cough**, and focal lung findings such as **crackles** or **dullness to percussion**, rather than predominantly bilateral wheezing. - Chest X-ray in pneumonia often shows **infiltrates** or **consolidation**, whereas in bronchiolitis, it commonly shows hyperinflation or peribronchial thickening. *Asthma exacerbation* - Asthma is uncommon as a first diagnosis in a child under **2 years of age**, especially in a **previously well** child with no history of recurrent wheezing episodes. - The **contact history with URI in a sibling** and the **acute, first-time presentation** strongly favor an infectious etiology (bronchiolitis) rather than asthma. - Asthma exacerbations typically occur in children with a known history of reactive airway disease and recurrent wheezing episodes.
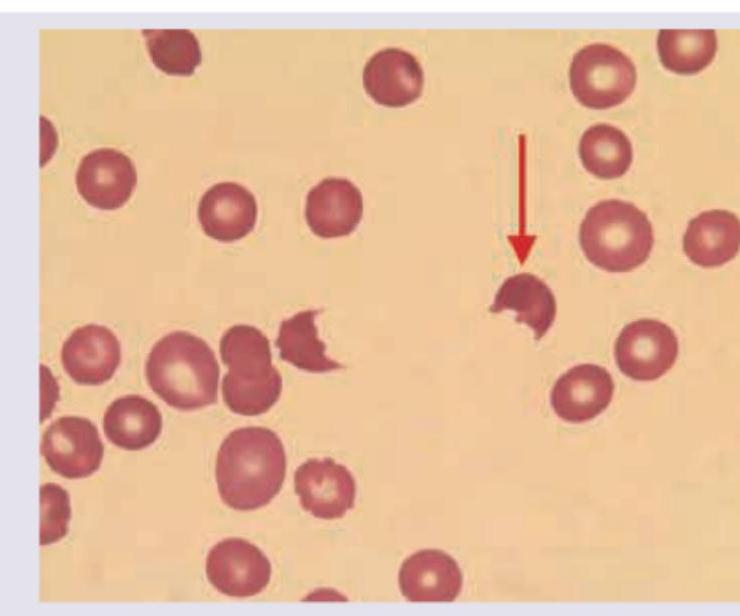
Question 9: A child with history of diarrhea 1 week back presents with sudden onset pallor and oliguria. Peripheral smear findings are shown below. Which of the following is unlikely finding in this disorder?
- A. Coomb's test negative
- B. Increased urinary sodium excretion
- C. Thrombocytopenia
- D. Elevated PT (Correct Answer)
Explanation: ***Elevated PT*** - **Hemolytic-uremic syndrome (HUS)** is a microangiopathic hemolytic anemia with **normal coagulation parameters**. - **PT** or **aPTT** are not typically elevated in HUS, making this an unlikely finding. *Coomb's test negative* - HUS is a **non-immune hemolytic anemia**, meaning the red cell destruction is not antibody-mediated. - A **negative Coombs test** is an expected finding in HUS, differentiating it from autoimmune hemolytic anemia. *Increased urinary sodium excretion* - HUS causes **acute kidney injury (AKI)**, often leading to tubular damage and impaired sodium reabsorption. - This can result in **increased fractional excretion of sodium** and high urinary sodium concentrations. *Thrombocytopenia* - **Thrombocytopenia** is a hallmark feature of HUS, caused by platelet consumption in the microthrombi formed in the damaged microvasculature. - The severity of thrombocytopenia can vary but is almost always present.
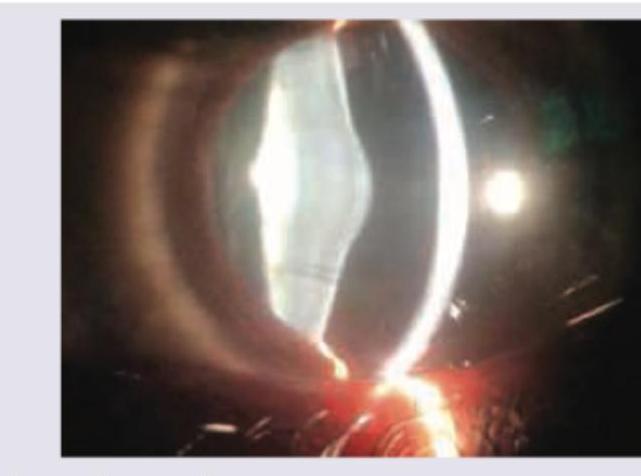
Question 10: A child during evaluation of recurrent hematuria has the following eye finding. He has sensorineural deafness and history of similar illness in family members. What is the diagnosis?
- A. IgA nephropathy
- B. Alport syndrome (Correct Answer)
- C. Thin glomerular basement membrane disease
- D. Post Streptococcal glomerulonephritis
Explanation: ***Alport syndrome*** - The combination of **recurrent hematuria**, **sensorineural deafness**, and a **family history of similar illness** is classic for Alport syndrome. - The image shows **anterior lenticonus**, a pathognomonic eye finding in Alport syndrome, which is a protrusion of the anterior lens capsule and cortex. *IgA nephropathy* - While associated with **recurrent hematuria**, it typically does not present with sensorineural deafness or specific ocular findings like **anterior lenticonus**. - Renal biopsy showing **IgA deposits** in the mesangium is characteristic. *Thin glomerular basement membrane disease* - This condition presents with **benign familial hematuria** and usually has a good prognosis, but it is not typically associated with **sensorineural deafness** or specific ocular abnormalities. - The glomerular basement membrane is uniformly thin on electron microscopy. *Post Streptococcal glomerulonephritis* - This is an **acute** condition following a streptococcal infection, characterized by **hematuria**, **edema**, and **hypertension**. - It is not a recurrent condition and does not involve **sensorineural deafness** or **anterior lenticonus**.