NEET-PG 2018 — Pathology
3 Previous Year Questions with Answers & Explanations
Which of the following hematological condition is shown below?
All are correct about the condition shown in the image except: (NEET Pattern 2018)
Which is not a true statement about this anomaly of kidney?

NEET-PG 2018 - Pathology NEET-PG Practice Questions and MCQs
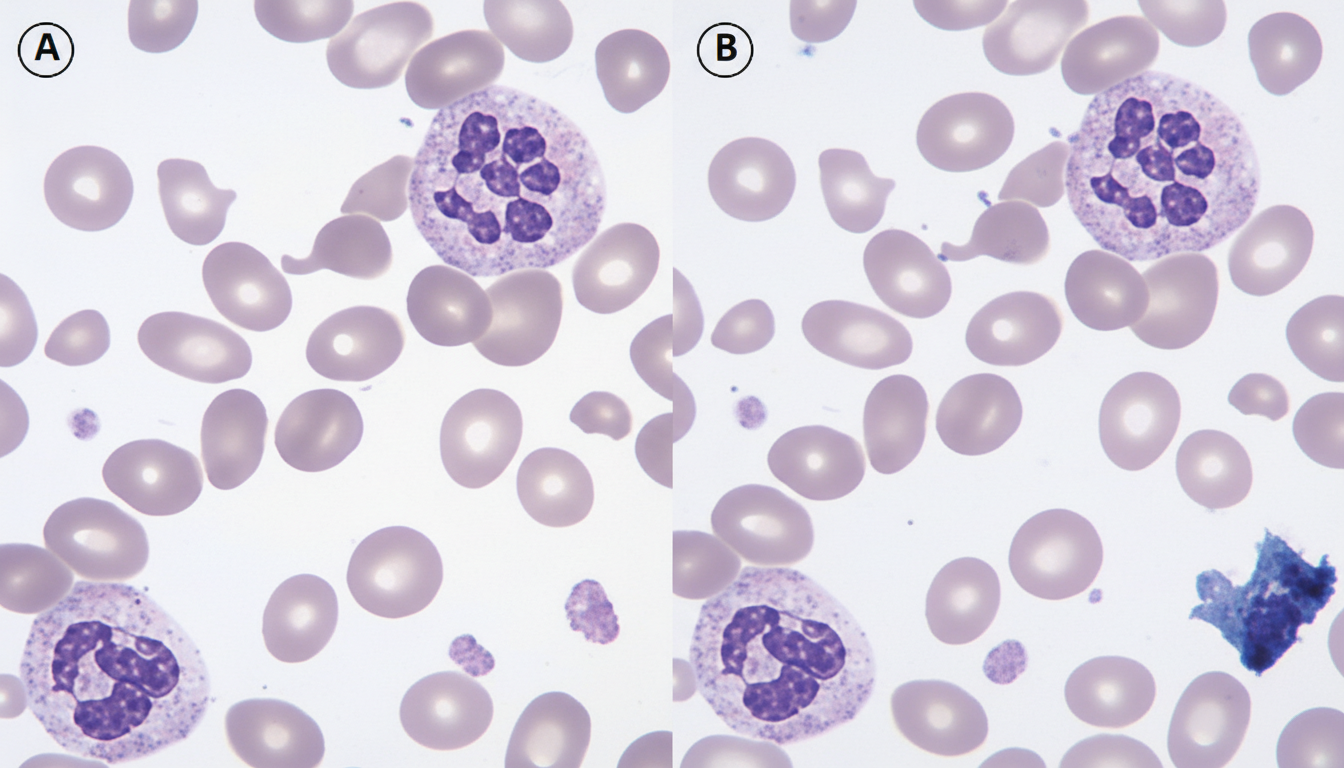
Question 1: Which of the following hematological condition is shown below?
- A. Multiple myeloma
- B. Megaloblastic anemia (Correct Answer)
- C. CML
- D. Metastasis
- E. Myelodysplastic syndrome
Explanation: ***Megaloblastic anemia*** - The image likely displays **hypersegmented neutrophils** and **macrocytic red blood cells**, which are characteristic features of **megaloblastic anemia** [1]. - This condition results from impaired DNA synthesis, often due to **vitamin B12** or **folate deficiency**. *Multiple myeloma* - This condition is characterized by the proliferation of **plasma cells** in the bone marrow, leading to **rouleaux formation** of red blood cells and **punched-out lesions** in bones [2]. - While rouleaux can be seen, the primary features of megaloblastic anemia (hypersegmented neutrophils, macro-ovalocytes) are distinct. *CML* - **Chronic Myeloid Leukemia (CML)** is a myeloproliferative neoplasm characterized by the presence of the **Philadelphia chromosome** (BCR-ABL fusion gene) [3]. - Peripheral blood smears typically show a **leukocytosis** with a full spectrum of myeloid maturation, including increased **basophils** and **eosinophils**, which are not the defining features of the image. *Metastasis* - **Metastasis** refers to the spread of cancer cells from a primary tumor to distant sites, often involving the bone marrow. - While bone marrow involvement can lead to various hematological abnormalities, the specific features of **hypersegmented neutrophils** and **macrocytic red blood cells** are not directly indicative of metastasis but rather of a primary hematological disorder like megaloblastic anemia. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 613-614. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, pp. 606-607. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, pp. 624-625.
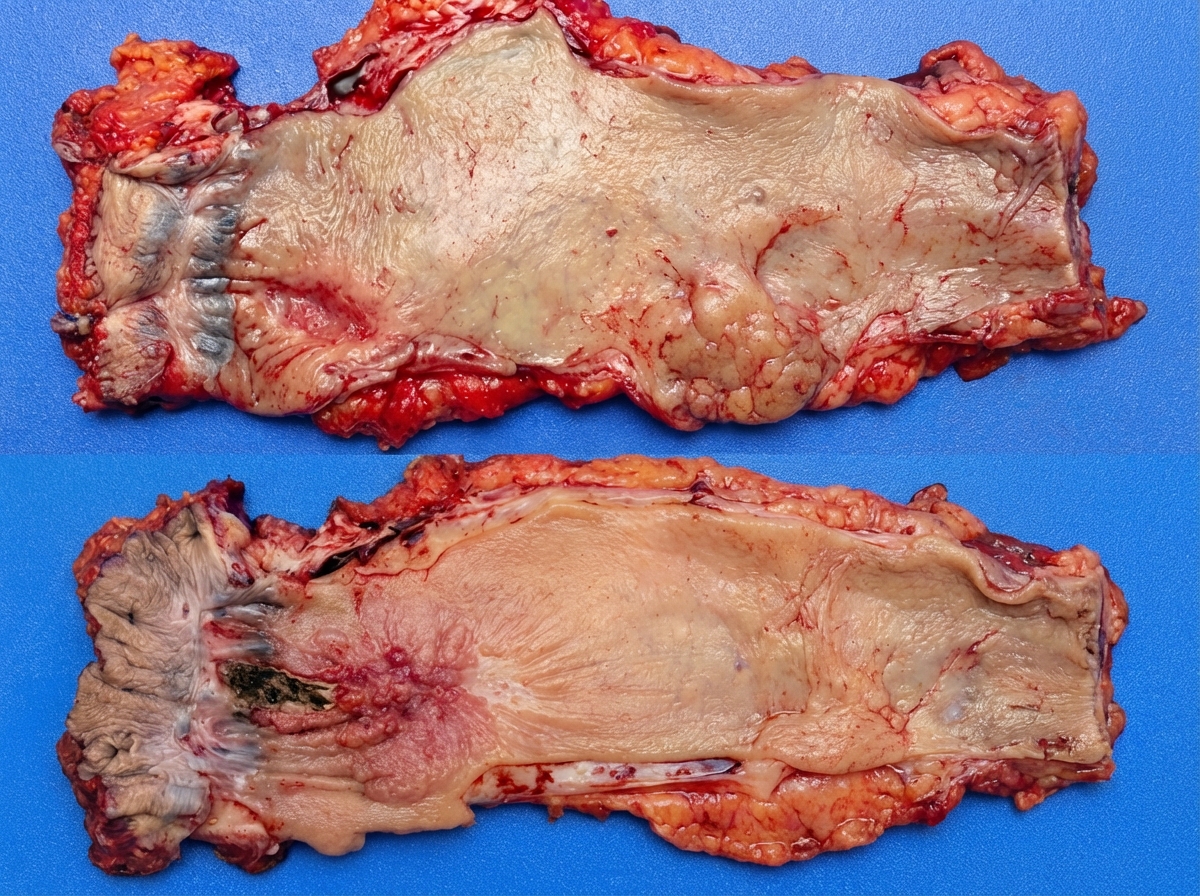
Question 2: All are correct about the condition shown in the image except: (NEET Pattern 2018)
- A. Most common site is middle esophagus (Correct Answer)
- B. Most common gross presentation is fungating subtype
- C. Stage 3 cancer oesophagus has 25 % survival rate
- D. Vomiting of previous day food items
- E. Loss of ganglion cells in myenteric plexus
Explanation: ***Most common site is middle esophagus*** - The question asks for the incorrect statement, and this statement is actually **correct** for esophageal squamous cell carcinoma (SCC), which is the most common type of esophageal cancer globally. - **Squamous cell carcinoma** of the esophagus most frequently occurs in the **middle third** of the esophagus [1]. *Most common gross presentation is fungating subtype* - This statement is incorrect. The most common gross presentation of esophageal carcinoma is the **ulcerative type**, followed by fungating and infiltrative types [1]. - **Fungating tumors** are exophytic and protrude into the lumen, but they are not the most common gross morphology. *Stage 3 cancer oesophagus has 25 % survival rate* - This statement is incorrect. The 5-year survival rate for **Stage III esophageal cancer** is significantly lower, typically ranging from **10-15%**, not 25% [2][3]. - Survival rates for esophageal cancer are generally poor, especially in advanced stages due to early metastasis and late presentation. *Vomiting of previous day food items* - This statement is incorrect. Vomiting of previous day's food items is characteristic of **pyloric stenosis** or **gastric outlet obstruction**, not typically esophageal cancer. - Esophageal cancer usually presents with **dysphagia** (difficulty swallowing) and **regurgitation** of recently ingested food, not undigested food from the previous day [3]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Gastrointestinal Tract, pp. 766-767. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Alimentary System Disease, pp. 349-350. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Gastrointestinal Tract, pp. 765-766.
Question 3: Which is not a true statement about this anomaly of kidney?
- A. Fusion of lower poles of the kidneys
- B. Association with Turner syndrome
- C. No risk of Wilms tumor (Correct Answer)
- D. Renal function usually is normal
- E. Associated with increased risk of renal calculi
Explanation: ***No risk of Wilms tumor*** - Horseshoe kidney, the anomaly described, actually has an **increased risk of Wilms tumor**, not no risk. - The risk is about 2-8 times higher than in the general population. *Fusion of lower poles of the kidneys* - This is the **classic anatomical description** of a horseshoe kidney, where the lower poles are fused across the midline [1]. - The fusion typically occurs at the **isthmus**, which can be fibrous or parenchymatous. *Association with Turner syndrome* - Horseshoe kidney is indeed **commonly associated with Turner syndrome** (XO karyotype). - Approximately 15-20% of individuals with Turner syndrome have a horseshoe kidney. *Renal function usually is normal* - In most cases, the **renal function of a horseshoe kidney is normal** [1], provided there are no other associated anomalies or complications. - However, they are more prone to complications like **hydronephrosis**, **calculi**, and infections due to altered anatomy. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 545-546.