All (366)Anatomy (27)Anesthesiology (4)Biochemistry (28)Biochemistry (1)Community Medicine (12)Dental (1)Dermatology (8)ENT (4)Forensic Medicine (3)General Medicine (3)Internal Medicine (41)Microbiology (25)Obstetrics and Gynecology (24)Ophthalmology (3)Orthopaedics (6)Pathology (35)Pathology (4)Pediatrics (22)Pharmacology (23)Physiology (13)Psychiatry (8)Psychiatry (3)Radiology (26)Surgery (8)Surgery (34)
Q41
Which of the following organisms is MOST associated with histamine production in scombroid fish poisoning?
Q42
A boy presented with multiple non suppurative osteomyelitis with sickle cell anaemia. What will be the causative organism?
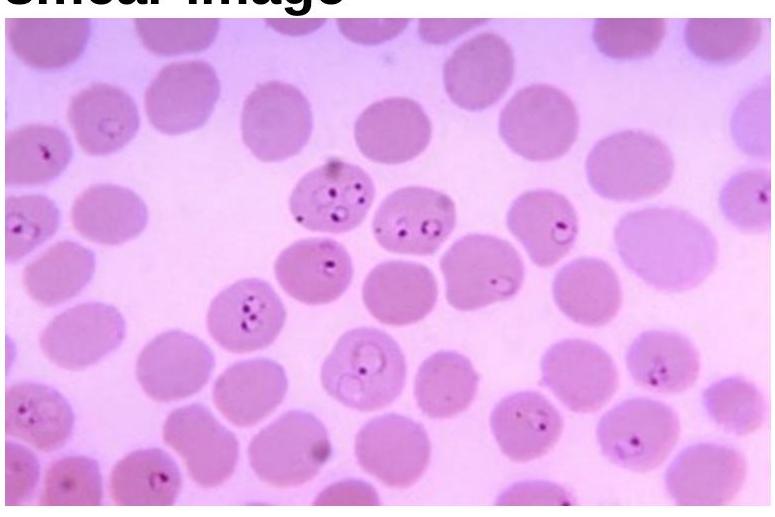
Q43
Identify the organism related to the blood smear image.