All (366)Anatomy (27)Anesthesiology (4)Biochemistry (28)Biochemistry (1)Community Medicine (12)Dental (1)Dermatology (8)ENT (4)Forensic Medicine (3)General Medicine (3)Internal Medicine (41)Microbiology (25)Obstetrics and Gynecology (24)Ophthalmology (3)Orthopaedics (6)Pathology (35)Pathology (4)Pediatrics (22)Pharmacology (23)Physiology (13)Psychiatry (8)Psychiatry (3)Radiology (26)Surgery (8)Surgery (34)
Q291
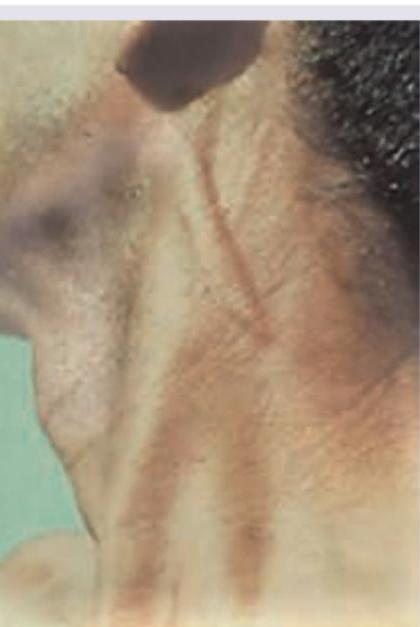
A 24-year-old male presents with a lesion at the site shown in the image for 4 years. He says it has increased in thickness over the years. Diagnosis is:

Q292
Which nerve is thickened in this patient of Hansen disease?
Q293
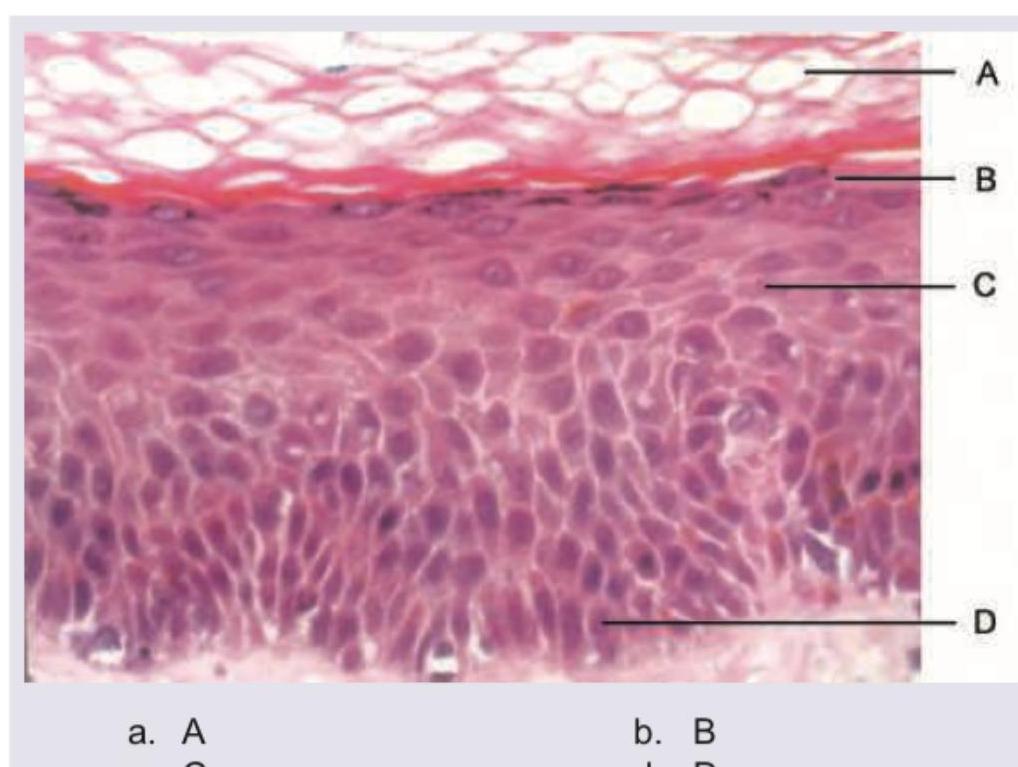
Which of the following layers is absent in psoriasis?