All (366)Anatomy (27)Anesthesiology (4)Biochemistry (28)Biochemistry (1)Community Medicine (12)Dental (1)Dermatology (8)ENT (4)Forensic Medicine (3)General Medicine (3)Internal Medicine (41)Microbiology (25)Obstetrics and Gynecology (24)Ophthalmology (3)Orthopaedics (6)Pathology (35)Pathology (4)Pediatrics (22)Pharmacology (23)Physiology (13)Psychiatry (8)Psychiatry (3)Radiology (26)Surgery (8)Surgery (34)
Q281
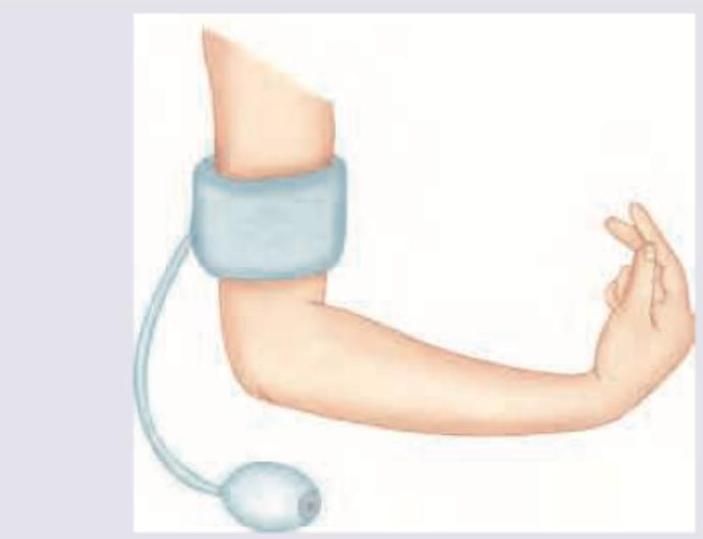
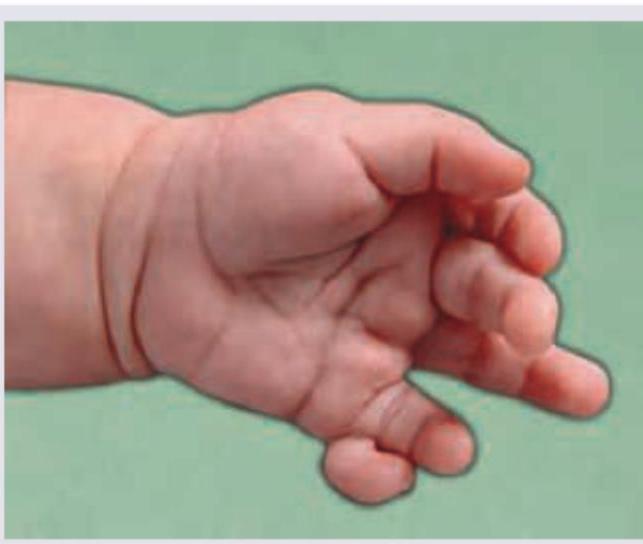
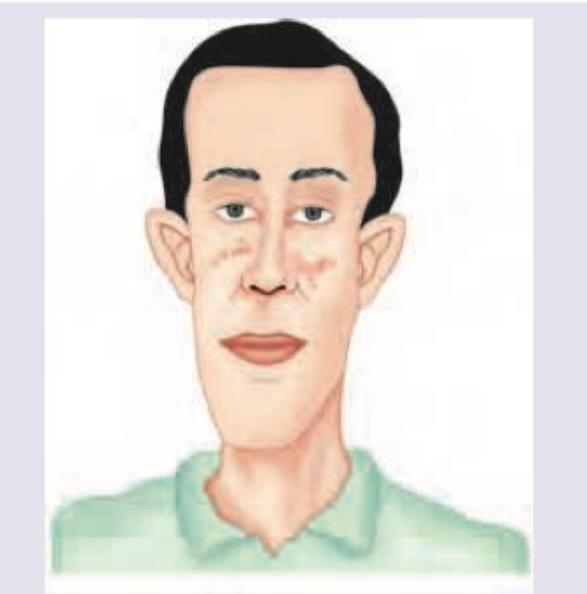
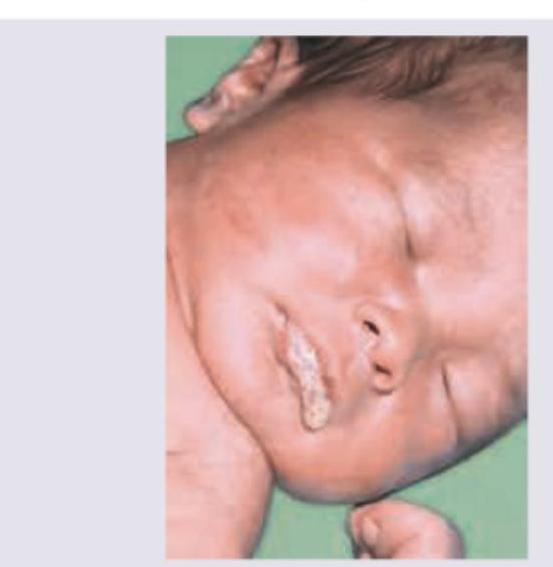
In a child with suspected tetany, the following test is performed. Identify the sign?