All (366)Anatomy (27)Anesthesiology (4)Biochemistry (28)Biochemistry (1)Community Medicine (12)Dental (1)Dermatology (8)ENT (4)Forensic Medicine (3)General Medicine (3)Internal Medicine (41)Microbiology (25)Obstetrics and Gynecology (24)Ophthalmology (3)Orthopaedics (6)Pathology (35)Pathology (4)Pediatrics (22)Pharmacology (23)Physiology (13)Psychiatry (8)Psychiatry (3)Radiology (26)Surgery (8)Surgery (34)
Q271
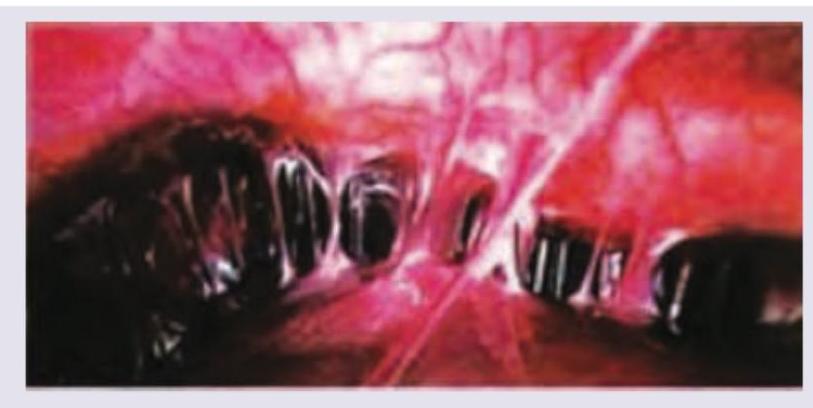
Which one of the following is implicated in the etiology of these adhesions around the liver?